Table 1 shows that during 2016-2017, 184 eyes from 94 white non-diabetic donors >80 years of age were recovered. The mean death-to-preservation time was 3.9 h (range: 2.0-6.4 h). Of the 184 eyes reviewed, 75 (40.2%) had certain AMD. The following categories were identified: Unremarkable (39.7%), Questionable (11.4%), Early-Intermediate AMD (22.8%), Atrophic (7.6%), Neovascular (9.8%), Other (8.7%), and Unknown/Not Recorded/Not Gradable (<1%). Figure 2, Figure 3, Figure 4, and Figure 5 show multiscale, multimodal ex vivo imaging of exceptionally well-preserved eyes from this series. The eyes were reviewed in collaboration with an ophthalmologist specializing in retinal disease (J.A.K.). While some eyes showed individual features better than others, these cases were chosen for all-around high quality.
As described38, ex vivo color photography differs from the corresponding in vivo photography. Retinal edema and/or detachment can reduce the visibility of the posterior pigmented tissues. Observations in fresh eyes indicate that these changes occur postmortem and do not worsen markedly with prompt fixation. In addition, choroidal vessels empty after death. Due to an undulating background of pale vessels and dark interstitial tissue, the assessment of pigmentary variations in the plane of the RPE should be assisted by modalities other than color. In ex vivo OCT, more information is available than in color photography. Ex vivo OCT also differs significantly from in vivo OCT. The major differences include the overall increased reflectivity of tissue, especially in the inner retina, the consistent reflectivity of some bands (nerve fiber layer, inner and outer plexiform layer, RPE), the lower visibility of the choroid details, especially under the edematous retina, and the visibility of tissue layer detachments (see below). The outer retinal hyperreflective bands, involving photoreceptors and the RPE (ellipsoid zone, EZ; interdigitation zone, IZ), are inconsistently visible ex vivo and are not used as landmarks in this context. The clinical consensus for spectral domain OCT uses the term RPE-Bruch's membrane (BrM) band. However, the term RPE-basal lamina (BL)-BrM band is preferred because it accommodates the appearance of basal laminar deposits in AMD24.
Figure 2 shows an unremarkable macula and hyporeflective large choroidal vessels, with a reflective RPE-BL-BrM band between the two. A large vessel in the inner retina casts a shadow on the posterior layers. The IPL and OPL are moderately reflective. In the NIR SLO, both the retinal and choroidal vasculatures are visible. The red-free reflectance SLO works best for features of the inner retina and vitreoretinal interfaces like the arcuate fibers and the papillomacular bundle of the NFL. In normal eyes, the 488 nm autofluorescence SLO shows an area of overall reduced signal in the central macula due to thickened parafovea and, in some cases, absorption by the yellow xanthophyll pigment, as well as hyperautofluorescence lining the large retinal vessels, which is suggestive of connective tissue sheaths. The autofluorescence at 787 nm shows a small region of increased signal in the central macula from the RPE, a signal in the choroidal stroma, and hypoautofluorescent stripes corresponding to the choroidal vessels.
Figure 3 shows a macula with early-intermediate AMD. The visible features include a soft drusen (dome-shaped RPE elevation near the fovea), SDDs (intermittent reflectivity with a dentate appearance internal to the RPE-BL-BrM band), hyper-reflective foci (HRF, reflective material with the same reflectivity as the in-layer RPE, located in the retina), and vitelliform change (an inward expansion of the RPE organelles, both intracellular and extracellular, in conjunction with basal laminar deposits39). The color photography shows strong pigmentation corresponding to the vitelliform lesion, surrounded by reduced pigmentation. Neither the drusen nor the SDDs are clearly visible by color. The NIR reflectance shows the reflectivity in the fovea. The autofluorescence at 488 nm excitation shows a mottled signal in the fovea. SDDs appear occasionally on SLO modalities; this is more likely if the SDDs are abundant, and SDDs are most easily seen as a regularly spaced punctate pattern (see Spaide and Curcio19, Figure 6). The pattern superior and temporal to the fovea in Figure 3I is not SDD, because it is irregular and localized to a superficial focal plane. All the en face modalities show fine folds radiating from the fovea. In less well-preserved eyes, similar folds may be large enough to be visible at the lowest viewing magnifications.
Figure 4 shows a macula with atrophic AMD. The color fundus photography shows circular atrophic areas, central hyperpigmentation, and small hyperpigmented dots in the parafovea that correspond in the OCT to HRF at the level of Henle fiber layer-outer nuclear layer (HFL-ONL). Additionally, in OCT, a low flat RPE elevation may represent a basal laminar deposit, non-exudative type 1 neovascularization, or both. Atrophy in the foveal B-scan is recognizable by the subsidence of the HFL-ONL, an area of hypertransmission (light shining through to choroid), a vitelliform change with increased shadowing in the foveal center, and HRF that cast shadows. In this eye, the NIR reflectance shows hyper-reflective spots in the fovea. The autofluorescence at 787 nm excitation effectively shows a signal corresponding to foveal hyperpigmentation and the absence of a signal in the circular atrophic areas. The red-free and 488 nm autofluorescence show the inner retinal features.
Figure 5 shows a macula with macular atrophy secondary to neovascular AMD. The color fundus photography shows black pigmentation within the atrophic area. The OCT shows atrophy by the sagging (subsidence) of HFL-ONL and increased hypertransmission. The foveal B-scan shows a mound of subfoveal hyperreflective material and intraretinal cysts. The near-infrared reflectance shows reflectivity in the atrophic area due to the loss of RPE and choroidal vessels. A small, intensely reflective area in the fovea is not visible on color. The red-free reflectance shows retinal vessels and, within an annular zone, choroidal vessels. The autofluorescence (488 nm) clearly shows a roughly circular atrophic border and islands of incipient atrophy. A central area devoid of signal is surrounded by an annulus of moderate signal and visible choroidal vessels.
Figure 6 shows common artifacts in ex vivo OCT imaging. Edema can be prominent in the inner retina, creating bulges and folds through the fovea (Figure 6A,I). Mechanical damage can occur with traction on the vitreous or by direct contact of the retina with the dissecting tools, which results in the dislocation of material and, sometimes, loss of that material (Figure 6F,G). Detachments can occur along multiple tissue planes and may represent relative tensile forces between the layers that also occur in vivo. Any detachment can widen further upon subsequent processing. The most common detachment is retinal (i.e., between the photoreceptor outer segments and the apical processes of the RPE) (Figure 6B–D,F–I). The apical processes may either detach from the outer segments or remain with the RPE cell bodies, as determined by histology. Retinal detachments may be large and billowing (Figure 6B,D,I) or narrow and barely discernible (Figure 6C,F,G). Bacillary layer detachment (BALAD40) was first seen in the laboratory and then later found in clinical OCT. BALAD is attributed to a split through the myoid portion of the photoreceptor inner segments, which leaves the ellipsoid portion of the inner segment and the outer segment attached to the RPE (Figure 6A,D,I). BALAD should not be mistaken for SDD in ex vivo OCT. A third detachment plane is the inner limiting membrane (ILM), and there is often residual reflective fluid between the ILM and the remaining retinal layers (Figure 6A,B,I). The least common detachment is between the choroid and sclera (Figure 6C). The fovea often exhibits cystoid spaces that should not be considered pathological without supporting evidence, such as signs of neovascularization (Figure 6H). In single B-scans, undulations of the RPE can give the impression of drusen. The 3D view of an OCT volume clarifies that these travel along the choroidal vessels (Figure 6E,J). Undulations may be due to differential volume changes between the vessels and intervening stroma after death and during fixation.
To calibrate the expectations for quality and to explore the limitations of ex vivo OCT, Figure 7 compares the in vivo imaging, ex vivo imaging, and histology of three clinically documented eyes with AMD. These three eyes were preserved differently from those in Figure 2, Figure 3, Figure 4, and Figure 5. To confirm the structural OCT reflectivity sources, which are subcellular41, the eyes in Figure 7 were preserved in 2.5% glutaraldehyde and 1% glutaraldehyde to allow high-resolution epoxy resin histology and correlative electron microscopy. Glutaraldehyde adds opacity to these specimens relative to those in Figure 2, Figure 3, Figure 4, and Figure 5. The effect of a shorter versus longer DtoP is apparent (Figure 7A–F, 2.1 h vs. Figure 7G–I, 8.9 h). In the eye with a longer DtoP, postmortem edema changed the retinal contour, and the ILM was detached. The pathology of interest (outer retinal tubulation) was subtle in the ex vivo imaging. It was found because the eye-tracked in vivo OCT pinpointed the relevant B-scan, and the choroidal vessels could be matched. In the two eyes with a shorter DtoP, some major pathologies (type 3 macular neovascularization) were immediately apparent (Figure 7A–C). Others were found with assistance from eye tracking (Figure 7D–F).
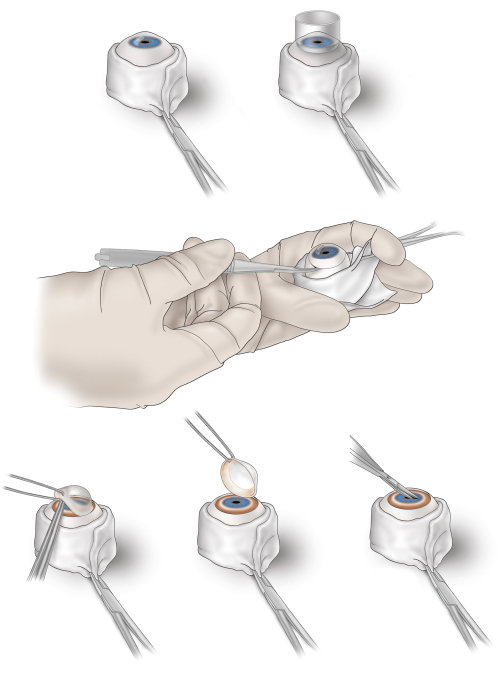
Figure 1: Corneal excision from a human donor eye for immersion fixation of the retina. Top left, the excised donor eye is held in place by a sheath of gauze stabilized by a hemostat; top right, an 18 mm trephine is used to make a circular score including the cornea and a 2 mm wide rim of sclera; middle, the scored circle is finished by a cut with spring-loaded curved tipped scissors, while the globe is stabilized; bottom left, the cornea and scleral rim are lifted, exposing the iris (blue) and ciliary body (tan-brown); bottom middle, the cornea with the rim is lifted off completely; bottom right, the iris is snipped perpendicular to the pupillary margin to facilitate the penetration of the preservative into the vitreous chamber. Please click here to view a larger version of this figure.
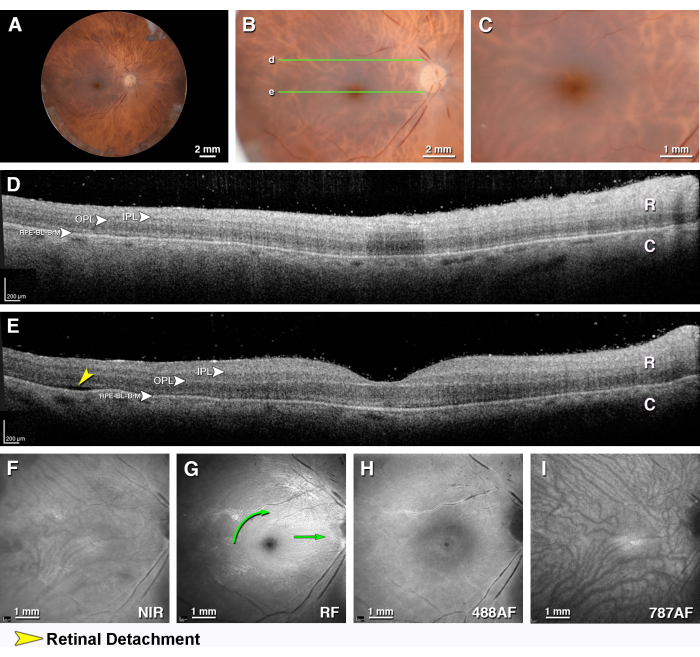
Figure 2: Multimodal ex vivo imaging of an unremarkable macula. A macula from an 82 year old female donor with a death-to-preservation interval of 1.97 h. (A) The fundus of the right eye viewed with the anterior segment removed (epi-illumination). (B) Close-up of the macula (epi-illumination). (C) Close-up view of the fovea (epi-illumination). The green lines indicate the locations of the OCT B-scans in panels D and E. (D,E) OCT B-scans through the (D) superior perifovea (E) and fovea. The retina (R), the choroid (C) with hyporeflective large vessels, and the intervening hyper-reflective RPE-BL-BrM band are visible. In this exceptionally well-preserved eye, the moderately reflective IPL and OPL are also visible. (D) A large vessel in the inner retina casts a shadow on the posterior layers. (E) The separation between the retina and RPE in panel E (yellow arrowhead) is artifactual. (F) The near-infrared reflectance shows the detail of both the retinal and choroidal vasculatures. (G) The red-free reflectance shows the arcuate fibers (left green curved arrow) and the papillomacular bundle (green arrow) of the nerve fiber layer. (H) The 488 nm wavelength autofluorescence shows an area of overall reduced signal in the central macula due to a thickened edematous parafovea, as well as rings and a point of low signal in the foveal center and hyperautofluorescence lining the large retinal vessels, which is suggestive of connective tissue sheaths. (I) The autofluorescence at 787 nm shows a small region of increased signal in the central macula from the RPE, a signal in the choroidal stroma, and hypoautofluorescent stripes corresponding to choroidal vessels. Please click here to view a larger version of this figure.
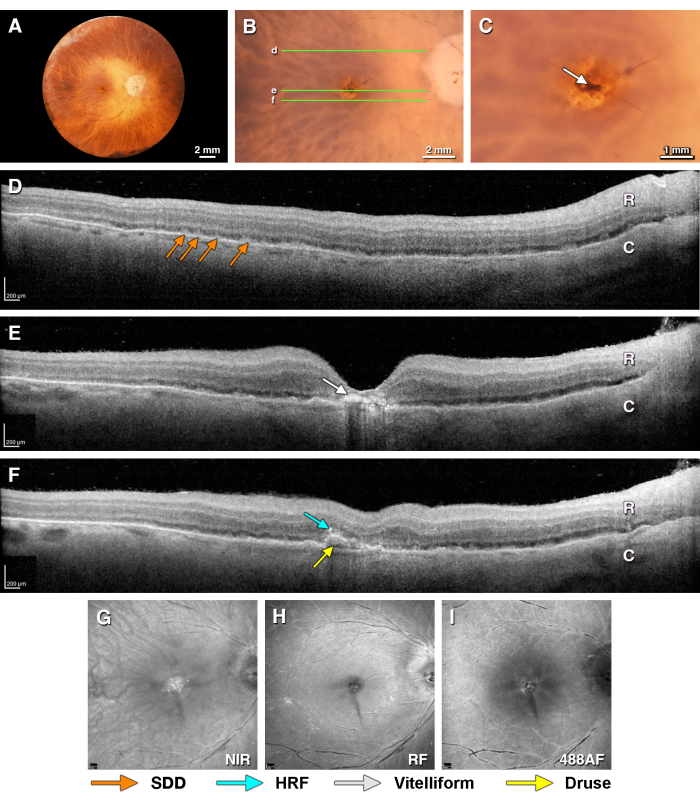
Figure 3. Multimodal ex vivo imaging of a donor eye with early intermediate AMD. Donor eye from a 97 year old female donor with a death-to-preservation interval of 3.1 h. (A) The fundus of the right eye viewed with the anterior segment removed (epi-illumination). (B) Close-up of the macula (epi-illumination). The green lines indicate the locations of the OCT B-scans in panels D, E, and F. (C) Close-up view of the fovea showing hyperpigmentation (arrow, flash illumination). (D) An SDD in the superior perifovea (orange arrows) is seen on OCT. I Vitelliform change in the RPE under the fovea (white arrows). (F) Inferior to the fovea is a soft drusen with a hyporeflective line at the base (yellow arrow) and a hyper-reflective focus above (light blue arrow). (G–I) The scanning laser ophthalmoscope images show very fine stellate folds in the fovea (also seen in C). (G) The near-infrared reflectance shows reflectivity material in the fovea corresponding in part to vitelliform material. (H) The red-free reflectance shows the retinal surface. (I) The 488 nm wavelength autofluorescence shows an area of overall reduced signal in the central macula due to a slightly thickened parafovea. SDDs are not clearly visible. Please click here to view a larger version of this figure.
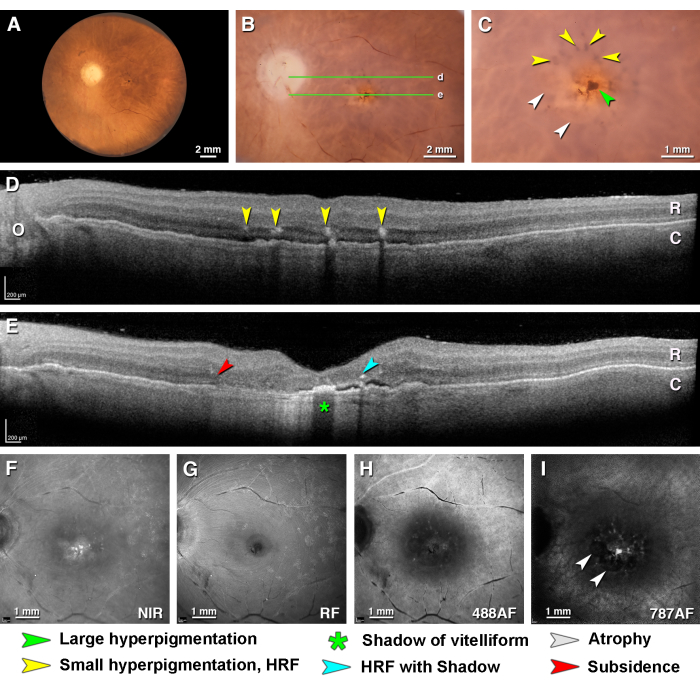
Figure 4: Multimodal ex vivo imaging of a complete RPE and retinal atrophy in age-related macular degeneration. Donor eye from a 97 year old female with a death-to-preservation interval of 2.33 h. (A) Fundus of left eye viewed with trans-illumination. (B) Close-up of the macula (epi-illumination). The green lines indicate the locations of the OCT B-scans in panels D and E. (C) Close-up of the fovea (epi-illumination) showing central hyperpigmentation (green arrowhead) and small hyperpigmented dots (yellow arrowheads). The central dot is intense brown because the overlying retina is very thin. The dots appear desaturated because the overlying retina is thick. Circular atrophic areas are indicated (white arrowheads). (D,E) OCT B-scans through the (D) perifovea (E) and fovea. The retina (R) and thin choroid (C) are visible. (D) Hyper-reflective foci (yellow arrowheads) at the level of the HFL-ONL correspond to the hyperpigmented dots in C. The low flat RPE elevation under them may represent a basal laminar deposit, non-exudative type 1 neovascularization, or both. (E) The B-scan through the fovea shows atrophy recognizable by the subsidence of the HFL-ONL (red arrowhead), an area of hypertransmission, a vitelliform change with increased shadowing in the foveal center (green asterisk), and hyper-reflective foci (teal arrowhead) with shadowing. The hyporeflective space between the retina and the RPE band may represent subretinal fluid. (F) The near-infrared reflectance shows hyper-reflective spots in the fovea. (G) The red-free image shows the arcuate fibers of the NFL and reflective blooms on the retinal surface. (H) The 488 nm autofluorescence focused on the retina shows a signal associated with the retinal vessels, no signal associated with the RPE, and faint autofluorescent spots in the central macular area. (I) The 787 nm autofluorescence shows a signal corresponding to pigmentation in C. Circular atrophic areas are apparent. Please click here to view a larger version of this figure.
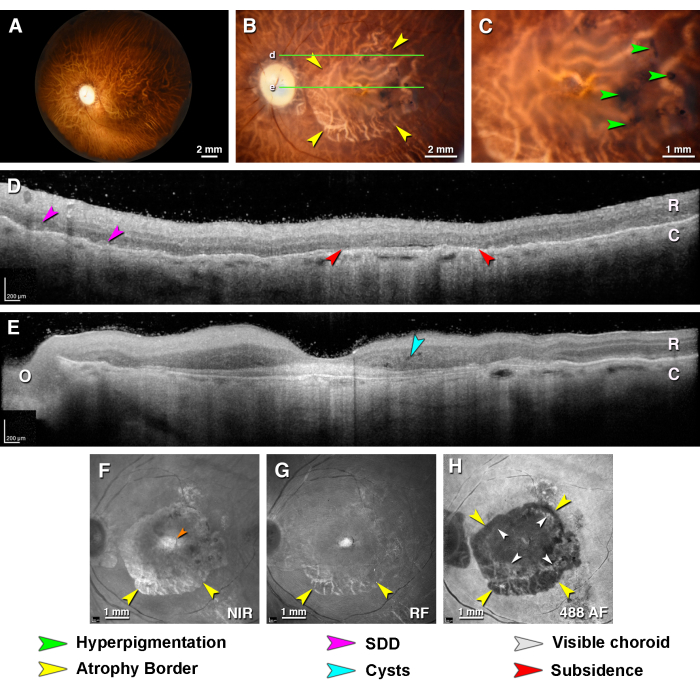
Figure 5: Multimodal ex vivo imaging of type 1 neovascularization and macular atrophy in age-related macular degeneration. A donor eye from an 86 year old female donor with a death-to-preservation interval of 3.5 h. (A) The fundus of the left eye viewed with the anterior segment removed (trans-illumination). (B) Close-up of the macula detailing atrophic borders (yellow arrowheads). The green lines indicate the locations of the OCT B-scans in panels D and E. (C) Close-up of the fovea shows black pigmentation (green arrowheads) within the atrophic area. (D,E) OCT B-Scans through the (D) perifovea (E) and fovea. The retina I and thin choroid (C) are visible. In this exceptionally well-preserved eye, the moderately reflective IPL and OPL are also visible. (D) The perifoveal B-scan grazes the superior edge of the atrophic area. Atrophy is evidenced by the sagging of the HFL-ONL and increased hypertransmission (red arrowheads). Possible subretinal drusenoid deposits are indicated (fuchsia arrowheads). (E) The foveal B-scan shows a mound of subfoveal hyper-reflective material and intraretinal cysts (asterisk). O = optic nerve head. (F) The near-infrared reflectance shows a reflective area of atrophy and choroidal vessels (teal arrowheads), including a small intense area in the central macula (orange arrowhead) not visible by color imaging. (G) The red-free reflectance shows retinal vessels and, within an annular zone, choroidal vessels. (H) The 488 nm autofluorescence depicts a roughly circular atrophic border (yellow arrowheads) and islands of incipient atrophy. A central area devoid of autofluorescence is surrounded by an annulus of moderate autofluorescence and visible choroidal vessels (white arrowheads). The 787 nm autofluorescence was not possible in this eye. Please click here to view a larger version of this figure.
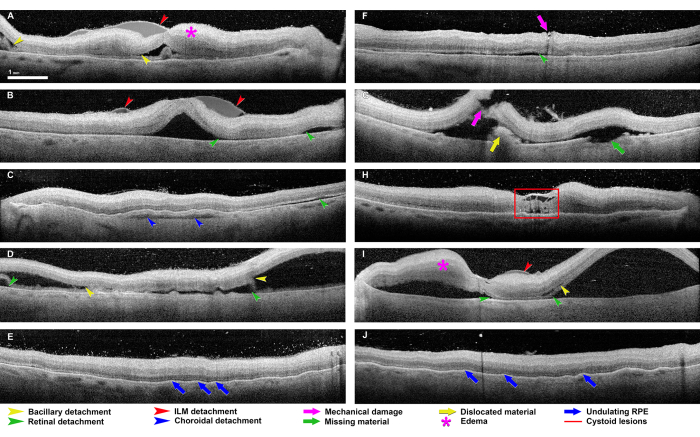
Figure 6: Common artifacts seen in the ex vivo OCT imaging of donor eyes. These eyes come from the 2016-2017 series of eyes. Most retinas are hyper-reflective relative to the retinas imaged in vivo, and the inner retinal layers are more reflective than the outer retinal layers. Bacillary detachment (yellow arrowheads in panels A, D, G, and I) is defined as a split at the level of the photoreceptor inner segment myoid, which creates a distinctive intraretinal cavity40. Retinal detachment (green arrowheads in panels B, C, D, F, G, and I) describes a separation of the entire neurosensory retina from the underlying RPE42. Detachments of the internal limiting membrane (ILM) separate the ILM and nerve fiber layer (red arrowheads in panels A, B, and I). A choroidal detachment (blue arrowhead in panel C) is a separation within the choroid or between the choroid and sclera. Mechanical damage (purple arrow in panels F and G) can appear at any level and with any dimensions, as applies to missing material (green arrow in panel G) and dislocated material (yellow arrow in panel G). The retinal edema (purple stars in panels A and I) appears as a thickening of the retinal tissue with poorly defined boundaries between the separate retinal layers. An undulating RPE (blue arrows in panels E and J) appears as an uneven, wavy RPE layer. Cystoid lesions (red square in panel H) correlate to hyporeflective chamber-like alterations within the retinal tissue, commonly in the fovea. Please click here to view a larger version of this figure.
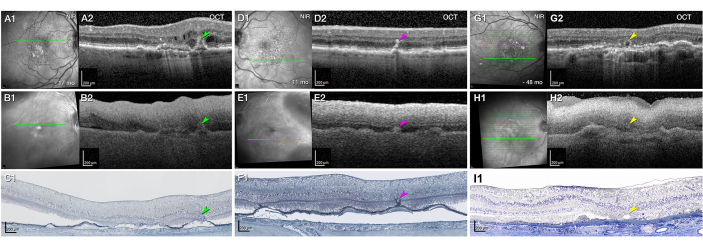
Figure 7: Ex vivo visibility of the pathology seen in vivo dependent on the preservation quality. (A–I) Panels A, B, and C, panels D, E, and F, and panels G, H, and I represent three clinically documented eyes from two donors, each seen by eye-tracking in vivo (A1–A2,D1–D2,G1–G2) and ex vivo (B1–B2,E1–E2,H1–H2) imaging, followed by histology (C,F,I). The green lines on the near-infrared reflectance (NIR, A1,B1,D1,E1,G1,H1) represent the levels of optical coherence tomography (OCT) B-scans and panoramic histology. Panels A, B, and C and panels D, E, and F, present the right and left eye, respectively, of one female donor in her 90s. Panels G, H, and I show the right eye of a second female donor, also in her 90s. (A–C) Well-preserved ocular tissue (DtoP: 2.1 h) enables good visibility of the major pathology. (A) A hyper-reflective intraretinal macular neovascularization (type 3 MNV, green arrowhead) is surrounded by intraretinal fluid 17 months before death (A2). The RPE/Bruch's membrane complex is split by hyporeflective material and appears as a "double layer" sign (A2). To the left is another double layer sign with barcode hypertransmission into the choroid (orange arrowhead). On ex vivo OCT (B2), the type 3 MNV and barcode hypertransmission are clearly visible and delineated. The retina is artifactually detached, as shown by the white arrowhead. The panoramic histology shows a vertically oriented type 3 MNV lesion (green arrowhead, C1). See previous research43,44 for details of the original case. (D–F) Well-preserved ocular tissue (DtoP: 2.1 h) can result in transparency that is reduced yet still sufficient for detecting major pathology. The OCT (D2) shows a stack of intraretinal hyper-reflective foci (HRF, fuchsia arrowhead) in an eye followed for exudative type 3 MNV. No intraretinal cysts are visible at 11 months before death. On ex vivo OCT (E2), the stack of HRF is compressed vertically (fuchsia arrowhead) but clearly delineated. On panoramic histology (F1), a retinal pigment epithelium tower (fuchsia arrowhead) rises upward from a soft druse. (G–I) Less well-preserved ocular tissue (DtoP: 8.9 h) results in reduced visibility of major pathology. The OCT indicates an outer retinal tubulation (ORT, yellow arrowhead) at 48 months before death (G2). On the ex vivo OCT, the ORT appears as a subtle disturbance, and this would have been difficult to discern without prior knowledge (H2). The inner limiting membrane is artifactually detached (white arrowhead). Edema has distorted the retinal contour. The histological analysis shows the ORT lumen delimited by the external limiting membrane and the photoreceptors protruding into it (I1). See previous research26,45 for details of the original case. Please click here to view a larger version of this figure.
| Numbers | Percentages | |||||
| Diagnostic category | Right Eyes | Left Eyes | Total | Right Eyes | Left Eyes | Total |
| Unremarkable | 39 | 34 | 73 | 41.50% | 37.80% | 39.70% |
| Questionable AMD | 10 | 11 | 21 | 10.60% | 12.20% | 11.40% |
| Early AMD | 20 | 22 | 42 | 21.30% | 24.40% | 22.80% |
| Atrophic AMD | 6 | 8 | 14 | 6.40% | 8.90% | 7.60% |
| Neovascular AMD | 11 | 7 | 18 | 11.70% | 7.80% | 9.80% |
| Other | 7 | 8 | 15 | 7.40% | 8.90% | 8.20% |
| Unknown | 0 | 0 | 0 | 0.00% | 0.00% | 0.00% |
| Not recorded | 1 | 0 | 1 | 1.10% | 0.00% | 0.50% |
| Total | 94 | 90 | 184 | 100.00% | 100.00% | 100.00% |
| Certain AMD | 37 | 37 | 75 | 39.40% | 41.10% | 40.20% |
| Possible AMD | 47 | 48 | 95 | 50.00% | 53.30% | 51.60% |
| Eyes were accessioned during the period 6/17/16 – 9/14/17. Criteria: ≥ 80 years, white, non-diabetic, ≤6 h death-to-preservation. Target: 184 eyes (180 eyes of 90 donors, preserved; 4 eyes of 4 donors, preserved) Death-to-preservation time (mean, maximum, minimum): 3.9 h, 6.4 h, 2.0 h | ||||||
Table 1: Donor eye recovery from 2016-2017.
Supplementary Material 1: Overview of the dissection, color fundus photography, and OCT-based multimodal imaging. Please click here to download this File.
Supplementary Material 2: Details of the OCT-based multimodal imaging to illustrate the steps in sections 5-8. Please click here to download this File.
