Glaucoma-inducing Procedure in an In Vivo Rat Model and Whole-mount Retina Preparation
Summary
Glaucoma is characterized by damage to retinal ganglion cells. Inducing glaucoma in animal models can provide insight into the study of this disease. Here, we outline a procedure that induces loss of RGCs in an in vivo rat model and demonstrates the preparation of whole-mount retinas for analysis.
Abstract
Glaucoma is a disease of the central nervous system affecting retinal ganglion cells (RGCs). RGC axons making up the optic nerve carry visual input to the brain for visual perception. Damage to RGCs and their axons leads to vision loss and/or blindness. Although the specific cause of glaucoma is unknown, the primary risk factor for the disease is an elevated intraocular pressure. Glaucoma-inducing procedures in animal models are a valuable tool to researchers studying the mechanism of RGC death. Such information can lead to the development of effective neuroprotective treatments that could aid in the prevention of vision loss. The protocol in this paper describes a method of inducing glaucoma – like conditions in an in vivo rat model where 50 µl of 2 M hypertonic saline is injected into the episcleral venous plexus. Blanching of the vessels indicates successful injection. This procedure causes loss of RGCs to simulate glaucoma. One month following injection, animals are sacrificed and eyes are removed. Next, the cornea, lens, and vitreous are removed to make an eyecup. The retina is then peeled from the back of the eye and pinned onto sylgard dishes using cactus needles. At this point, neurons in the retina can be stained for analysis. Results from this lab show that approximately 25% of RGCs are lost within one month of the procedure when compared to internal controls. This procedure allows for quantitative analysis of retinal ganglion cell death in an in vivo rat glaucoma model.
Introduction
Glaucoma is a group of eye diseases affecting neurons in the retina, specifically, the retinal ganglion cells1-2. The axons of these cells converge to become the optic nerve carrying visual information to the brain where vision is perceived. Damage to RGCs and their axons therefore causes visual defects.
The primary characteristics associated with glaucoma disorders are RGC degeneration and death, increased intraocular pressure (IOP), and optic disk cupping and atrophy. These features lead to visual field loss or complete, irreversible blindness. Currently, glaucoma has caused blindness in 70 million people worldwide 3. As such, it is the world's third largest cause of blindness 4.
The exact mechanism of RGC death in glaucoma remains unknown. Much research has been done to unlock the mystery. It is known, however, that the primary risk factor of glaucoma is an increase in intraocular pressure due to irregular circulation of aqueous humor (AH) in the anterior chamber of the eye. AH acts as a transparent and colorless replacement for blood in the avascular anterior chamber of the eye. It nourishes the surrounding cells, removes secreted waste products from metabolic processes, transports neurotransmitters, and permits the circulation of drugs and inflammatory cells within the eye during pathological states 1.
The maintenance of aqueous humor circulation involves the ciliary body and the trabecular meshwork. Aqueous humor is produced by the ciliary body. It then flows into the anterior chamber to maintain the overall health of the ocular tissue. 75 – 80% of aqueous humor outflow is actively secreted through non-pigmentary ciliary epithelium when the fluid is filtered through three layers of spongy tissue in the ciliary muscle. The fluid exits through the trabecular meshwork and through Schlemm's Canal which empties into the blood system 5.The remaining 20 – 25% of outflow bypasses the trabecular meshwork and is passively secreted by ultrafiltration and diffusion through the uveo-scleral pathway. This pathway appears to be relatively independent of intraocular pressure 1.
When aqueous humor production and outflow are out of balance, pressure builds within the eye. As stated, this increase in intraocular pressure is the primary risk factor in the development of glaucoma. Such pressure causes damage to the intricate layers of neurons in the retina at the back of the eye. Damage to the retinal ganglion cell axons of the optic nerve causes the brain to no longer receive accurate visual information. As a result, the perception of vision is lost and complete blindness can occur.
To date, there is no cure for glaucoma. Different treatment methods exist that primarily aim to reduce intraocular pressure. These include topical medication classes such as beta1-adrenergic receptor blockers, or topical prostaglandin analogues. Beta blockers reduce the intraocular pressure by decreasing the production of aqueous humor 7. Prostaglandins function to reduce IOP by increasing the outflow of aqueous humor 8-14. Alpha adrenergic agonists and carbonic anhydrase inhibitors are also used as secondary methods of treatment. Alpha adrenergic agonists increase outflow through the uveoscleral pathway 15-17. Carbonic anhydrase inhibitors reduce the production of AH by enzymatic inhibition 18. Much more invasive procedures are also being used to treat glaucoma. Laser trabeculoplasty is used to increase the outflow of aqueous humor 19. Another surgical therapy, called trabeculectomy, creates an alternative drainage site to filter AH when the traditional trabecular pathway is blocked 20-21.
These treatment options have been known to effectively reduce IOP. However, up to 40% of glaucoma patients show normal IOP levels indicating a need for more complete therapeutic methods.22,23 Additionally, retinal ganglion cell death seen in glaucoma is irreversible once it begins and current treatments do not stop the progression of the disease 24-28. This has highlighted the need for effective neuroprotective therapies that target the survival of the neurons themselves. Development of glaucoma models is crucial for this development.
In this study we are demonstrating a method of inducing glaucoma-like effects in adult Long Evans rats using a modified procedure originally outlined by Morrison29. In this procedure, injections of 2 M hypertonic saline into the episcleral venous plexus induces glaucoma-like conditions by scarring tissue to reduce aqueous humor outflow in the trabecular meshwork leading to an increase in intraocular pressure and a significant loss of RGCs within one month of the procedure 30-31. Glaucoma-inducing procedures, such as the one described here, may be the key to unlocking new developments in glaucoma treatments.
Protocol
All procedures using animal subjects have been in accordance with the standards of the Institute of Animal Care and Use Committee (IACUC) at Western Michigan University.
1. Animals
- Use male and female rats 3 months of age in this study.
- Keep animals in a 12 hr light/dark cycle with free access to food and water.
2. Preparation of KAX Cocktail for Animal Anesthesia
- Dissolve 50 mg of xylazine (20 mg/ml) in 5 ml ketamine (100 mg/ml) with 1 ml acepromazine (10 mg/ml) and 3 ml of distilled water. Mix thoroughly.
- Sterilize with a syringe filter and store this solution into a 10 ml serum bottle.
3. KAX Injection
- Weigh animal (g) and return to cage until ready for injection.
- Inject 0.1 ml KAX/100 g animal body weight intraperitoneally, using a 1 ml insulin syringe with a 28 G needle.
- Allow for animal to become unconscious. Check reflexes by pinching the feet and tail.
- Keep all animals safely in lab for the duration of surgery.
- Post-surgery, replace animals into their cages and keep comfortable in RT until consciousness is regained. Only return animals to the animal facility when the animals awaken and resume normal behavior.
4. Preparation for Surgery and Microneedle Assembly
- Make a sterile 2 M NaCl solution.
- Use a microelectrode puller (Figure 1C) to pull one 0.86 mm inner diameter heavy polished standard and thin walled borosilicate tube into two finely tapered glass microneedles (Figure 1D, Figure 1E).
- Backfill one microneedle from the previous step with 2 M saline using a backfilling syringe needle and a 1 ml syringe (Figure 1B) . Tap out air bubbles from the tip of the electrode.
- Fill a second 1 ml syringe with 2 M NaCl. Connect an 18 G needle and then attach a length (approximately 10 inches) of polyethylene tubing (Figure 1A). Use the syringe plunger to fill the polyethylene tubing with saline through the needle.
- When both the microneedle and tubing are filled with saline, carefully connect the two. Eliminate any air in the connection between them (Figure 2).
- Finely bevel the tip of the microneedle by scraping it very lightly against the grain of a course paper towel.
- Check the resistance of the microneedle by gently pushing the plunger on the syringe until a fine stream of liquid can be seen on the paper towel. The stream of liquid should be no wider than 0.5 mm.
5. Preparation of Animal
- Apply 1 – 2 drops topical anesthetic to cornea (Proparacaine Hydrochloride Ophthalmic Solution, USP, 0.5%). Wait until no ocular reflex occurs.
- Trim whiskers with scissors.
- Saturate a cotton tip applicator with betadine solution and swab area around the experimental eye.
- Using a microscope, attach a hemostat to clamp the bottom eyelid to bulge the eye, expose the episcleral vein and restrict eye movement. (Figure 3, arrowhead)
6. Glaucoma-inducing Saline Injection
- When the microneedle assembly and the animal are prepared, begin injections.
- When the animal is confirmed to be unresponsive to feet/tail pinch, carefully pierce the episcleral vein with the microneedle by coming at a low angle between 10 and 20 degrees to the vein (Figure 3, white arrow). A successful puncture into the vein is apparent when blood enters the tip of the microneedle (Figure 3, black arrow).
- Slowly and manually inject approximately 50 µl saline into the vein. This should take approximately 10 sec. The veins will blanch white as the salt circulates through the vasculature (Figure 4, arrowhead). Some regions may maintain a blood red appearance (Figure 4, arrow).
- Perform a second injection into the vein, opposite to the site of the first, to ensure thorough retinal damage to the complete retinal ganglion cell layer.
Note: Within minutes, one should see a distinct cloudy appearance through the iris of the eye as the salt circulates through the vascular system.
- Perform a second injection into the vein, opposite to the site of the first, to ensure thorough retinal damage to the complete retinal ganglion cell layer.
- Leave the opposite eye untreated for use as an internal control.
7. Animal Recovery
- Remove the hemostat.
- Use a cotton applicator to apply triple antibiotic ointment (Bacitracin zinc, neomycin sulfate, polymysin B sulfate) to the site clamped by the hemostat and to injection sites. Tissue damage around the eye does not occur using the hemostat.
- >Place anesthetized animals in their cages on a circulating warm water blanket to prevent hypothermia. Keep animals under observation until consciousness and normal behavior are regained. Transport awake animals back to the animal colony. Animals remain in the colony until the time of sacrifice.
8. Animal Sacrifice and Retina Removal
- One month following the procedure to induce glaucoma, animals are euthanized by CO2 asphyxiation and secondary thoracic puncture.
- Place the animal in the chamber and put the lid on securely.
- Open the CO2 and gas regulator valves to allow 20% volume/min CO2 displacement of oxygen in the chamber.
- Allow four to 5 min for the animal to expire.
- Turn off both valves.
- Remove animal from the chamber and perform a secondary thoracic puncture with a sterile scalpel.
- After euthanasia, use a scalpel to cut the connective tissue in the orbital cavity surrounding the eye, being careful not to cut into the eyeball itself.
- Carefully use curved edge scissors to cut the optic nerve and any remaining tissue to extract the intact eyeball. Place extracted eyeball in a sterile 60 mm x 15 mm disposable petri dish containing fresh PBS.
- Make an eyecup from the eyeball. To do this, make a small incision with the scalpel just posterior to the border between the iris and the sclera. Follow this incision around the circumference of the eye with small spring scissors to remove the corneal hemisphere from the eyeball. The hemisphere connected to the optic nerve remains.
- Find the very thin pink/beige retina inside the eyecup from the euthanized animal. Hold the pigmented layer of the retina with blunted forceps to stabilize the eyecup. Use another pair of closed forceps to very gently tease the whole intact retina off of the back of the eye. Avoid pinching, pulling, or tugging the retina directly.
- Use small spring scissors to cut the area where the optic nerve is still attached to the retina.
- Be sure to cut away any residual pigment epithelium or scleral tissue from the retina.
- Using a transfer pipette, very gently transfer the isolated retina to a clean sylgard coated 35 mm x 10 mm petri dish containing fresh PBS.
9. Whole-Mount Retina Preparation
- Once in the sylgard dish, use forceps and one cactus needle to pin the retina in place. Keep the retinal ganglion cell layer facing up and optic nerve down. The retina's hemispherical shape is notable even after fixation. The curvature of the retina will curl toward the ceiling when the retinal ganglion cell layer is in the desired orientation.
- Use small scissors to cut the retina into four quadrants, making the shape of a four leaf clover radiating from the optic nerve head.
- Pin the quadrants of the retina with additional cactus needles to make the retina as flat as possible without stretching (Figure 5).
- Fix the pinned retinas in the sylgard dish with 3 ml of 4% paraformaldehyde O/N at RT.
10. Antibody Staining of Retina
Note: Stain fixed retinas with primary and secondary antibodies for viewing neurons in the retina (Figure 6).
- Rinse fixed, flat-mounted retinas three times for 2 min each in PBS.
- Permeabilize the retinas with 1% Triton X-100 with 1% fetal bovine serum in PBS for 60 min.
- Rinse retinas three times, 2 min each, in PBS.
- Rinse twice with 0.1% Triton X-100 in PBS, 5 min per wash.
- Rinse twice with PBS, 5 min per wash.
- Incubate with 1% Triton X-100 and 1% fetal bovine serum in PBS at RT for 45 min.
- Rinse twice with 0.1% Triton X-100 in PBS, 5 min per wash.
- Rinse twice with PBS, 5 min per wash.
- Incubate each retina in 3 ml 1% fetal bovine serum in PBS with purified mouse anti-rat CD90/mouse CD90.1 (1:300 dilution) O/N at RT.
- Rinse retinas once with 0.1% Triton X-100 in PBS for 5 min.
- Rinse twice with PBS, 5 min per wash.
- Incubate each retina in 3 ml PBS (no FBS) with secondary Alexa Fluor 594 goat anti-mouse IgG (1:300) O/N at RT.
- Wash retinas with PBS liberally.
- Using a dissecting microscope, carefully remove cactus needles from the retina.
- Gently transfer retinas onto microscope slides with a transfer pipette. Be sure to maintain orientation with retinal ganglion cell layer facing to the ceiling. The retina's hemispherical shape is notable even after fixation. The curvature of the retina will curl toward the ceiling when the retinal ganglion cell layer is in the desired orientation.
- Absorb any excess PBS with KimWipe or other such absorbent material. Be careful not to absorb the retina.
- Add 5 drops of ½ glycerol and ½ PBS by weight as a mounting media.
- Cover retina with coverslip, avoiding air bubbles.
- Secure coverslip using clear nail polish, glue, or other adhesive.
Representative Results
This section illustrates the apparatus components and procedure used to induce glaucoma-like conditions in an in vivo rat glaucoma model. We show the individual tools and equipment used to perform a hypertonic saline injection which causes an increase in intraocular pressure. We show the injection into the episcleral venous plexus with its characteristic blanching effect and the cloudy appearance of the anterior chamber that results. We also describe the process of retina removal and flat-mounting for analysis of lost RGCs. Lastly, we show the effects of the injection on retinal ganglion cell survival. As the distribution of RGCs is uneven in different regions of the rat retina, images are obtained from four 200 µm2 regions in each retina, 4 mm away from the center of the optic nerve head. The total number of Thy 1.1 labeled RGCs in each section are counted, averaged and compared in experimental and control retinas 31. Using this method, RGC counts changed from an average of 225 in an image of control untreated conditions to 168 one month after the procedure to induce glaucoma-like conditions (N = 30). Taken together, the procedures outlined here can be followed step by step to analyze the death of retinal ganglion cell bodies and axons.
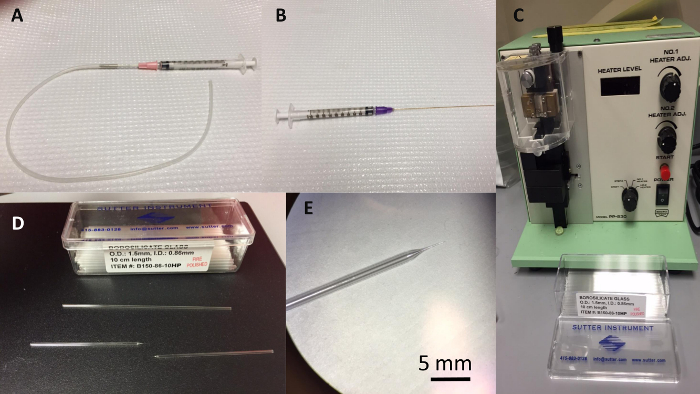
Figure 1. Microneedle Components. (A) Syringe with polyethylene tubing used for saline injection. (B) Backfill syringe used to backfill the borosilicate microneedle. (C) Narishige electrode puller used to make borosilicate microneedles. (D) Borosilicate glass electrodes before and after being pulled in the electrode puller. (E) Magnified view of microelectrode needle tip after being pulled. Please click here to view a larger version of this figure.
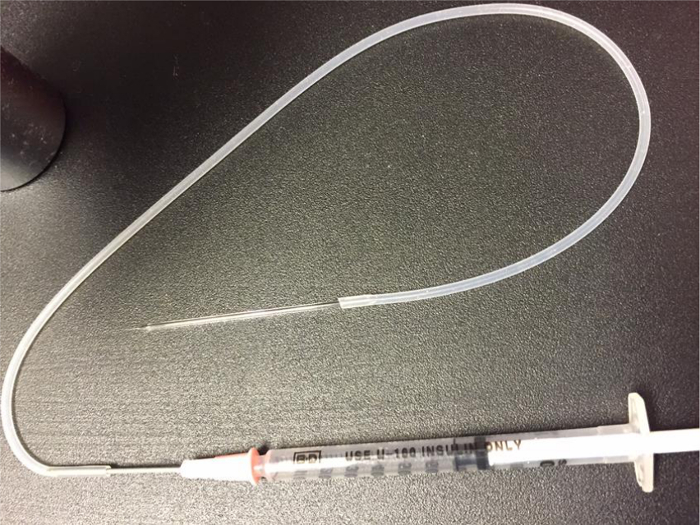
Figure 2. Complete Microneedle Assembly. Microneedle attached to polyethylene tubing attached to syringe with hypertonic saline. Please click here to view a larger version of this figure.
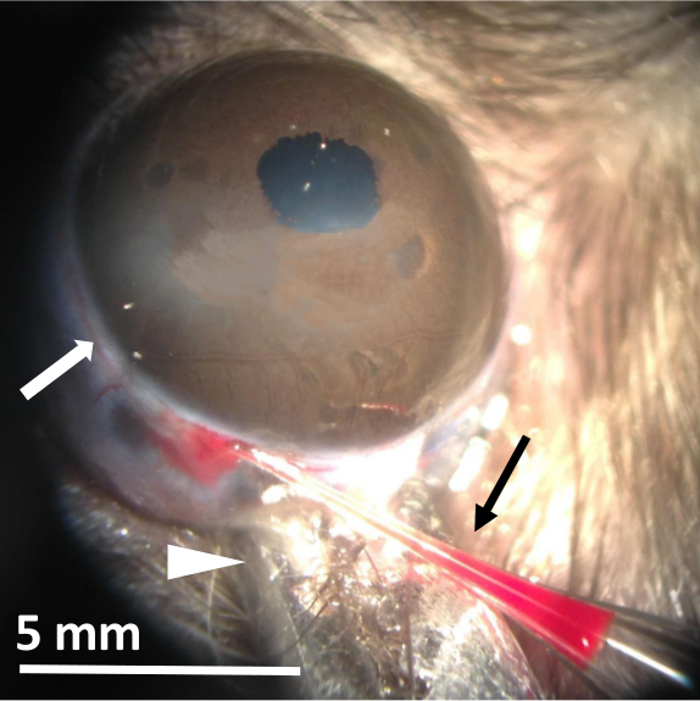
Figure 3. Glaucoma-inducing Saline Injection into the Episcleral Venous Plexus. Image of saline injection into the episcleral vein of a live, anesthetized Long Evans rat. The arrowhead indicates the location of the hemostat used to bulge the eye and prevent its movement. The white arrow indicates the location of the injected vein. The black arrow shows blood back flowing into the microneedle tip indicating successful vein puncture. Please click here to view a larger version of this figure.
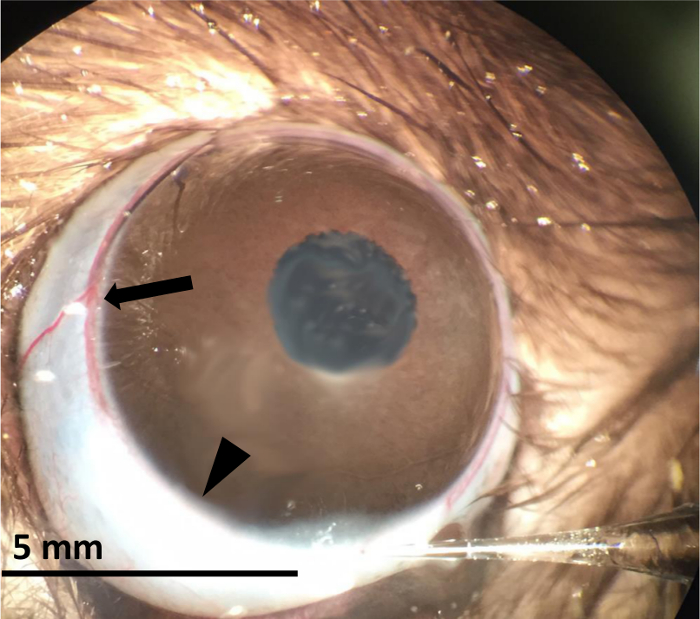
Figure 4. Blanching Effect of Hypertonic Saline Injection. Image of rat eye being injected with hypertonic saline. The arrowhead shows the characteristic blanching effect of saline in the episcleral venous plexus. The arrow indicates a portion of the episcleral venous plexus that has not yet blanched. Please click here to view a larger version of this figure.

Figure 5. Flat-mount of Rat Retina. Image of whole mount retina removed from the rat eye and pinned flat in a sylgard dish using cactus needles. The black arrow indicates the optic nerve head. Please click here to view a larger version of this figure.
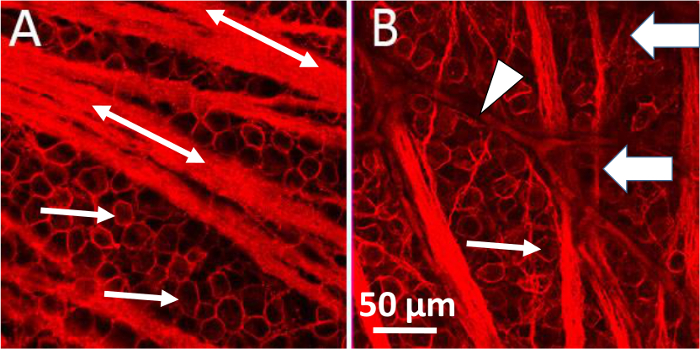
Figure 6. Damage to Retinal Ganglion Cells after Glaucoma-inducing Surgery. Comparison of control untreated eye (A) to experimental eye (B) one month after receiving glaucoma inducing saline injection. Retinas were labeled with an antibody against the RGC marker, Thy 1.1 (CD90). Thin arrows indicate individual RGCs in both the control and experimental conditions. The procedure leads to a reduction in the number of RGCs, defasciculation of the axons off the main axon bundles, and distortion to the circularity of remaining RGCs. Block arrows indicate the characteristic defasciculating axons resulting from the saline injection. The arrowhead shows a blood vessel within the retina. Double-ended arrows label axon bundles. Please click here to view a larger version of this figure.
Discussion
This protocol describes a method of inducing glaucoma-like conditions in an in vivo rat model. This procedure uses an injection of hypertonic saline to induce scarring in the trabecular meshwork 29, 32. Developing scar tissue occludes the outflow of aqueous humor which increases pressure in the anterior chamber. With decreased outflow and pressure build up, the lens suspended by elastic ligaments pushes back into the vitreous chamber. Vitreous humor then applies pressure onto the retina damaging the fragile retinal neurons. Our results using this procedure show that retinal ganglion cell numbers begin to dwindle at 2 weeks with significant loss of ganglion cell loss at 1 month post-procedure.
This protocol is only one method of inducing glaucoma in rodents. There are many other experimental models in which damage to retinal ganglion cells is accomplished either by an increase in intraocular pressure or by direct damage to the optic nerve 30. Often, these methods have been developed in larger animals and modified for application to mice and rats 33. Intraocular injections of toxins such as staurosporine 34 and NMDA, the non-hydrolyzable glutamate analog 35 induce rapid retinal ganglion cell death. Studies have shown, however, that such toxins follow a dose-response curve in mice and effect cells other than the target ganglion cells 35. Additionally, the damage to retinal ganglion cells in this model is much more direct than the gradual progression of human glaucoma.
Direct damage to the optic nerve can also be inflicted. Laser axotomy is a common way to sever the axons making up the optic nerve in mice 36. However, this method presents some complications. The small size of rodent orbits makes it difficult to accurately damage the optic nerve without affecting blood flow through the central retinal artery and vein. To overcome this, some researchers utilize a more invasive approach involving the removal of a small portion of brain in order to provide better access to the optic nerve 37. Optic nerve crush models access the optic nerve intraorbitally as well. In this model, the nerve is pinched by self-closing forceps and ocular blood flow is not compromised. This procedure results in an immediate insult and synchronous death of retinal ganglion cell. Studies using this model show significant loss of RGCs 38. However, some argue that it may induce more damage than that caused by elevated IOP alone 39. Additionally, glaucoma is characterized by slow, chronic, asynchronous loss of retinal ganglion cells 33, 39-42.Therefore, the time course and underlying mechanism of damage inflicted with optic nerve crush could be quite different than that occurring in human glaucoma. In contrast, the model discussed in this paper avoids the need for direct access to the optic nerve, eliminates any dissection of brain tissue, and allows for gradual retinal ganglion cell damage.
Microbead occlusion models of glaucoma use polystyrene or magnetic beads injected into the anterior chambers of rats or mice to elevate IOP. Most of this work has been done in mice and they show only a low to moderate level of damage in the optic nerve with wide variation in the results and inconsistent data 43-50. When using rats, the duration of elevated IOP was too short to cause enough damage to cells 48. Even with modifications to the procedure, the model still caused severe damage in short duration representing an acute neuropathic model rather than a chronic glaucoma model 51. Smedowski et al 43 have recently developed a further modified microbead procedure using an additional initial 'high pressure injury' to achieve longer lasting IOP elevation with chronic damage that does show promise. More studies using this technique are necessary to further validate this model.
Models of chronic ocular hypertension aim to obstruct aqueous humor outflow. Laser photocoagulation of the episcleral and limbal veins 52 and episcleral vein occlusion 53 are two such methods. However, it has also been shown that laser ablation techniques produce only transient IOP elevation and a moderate level of actual cell loss 36, 54-55.
Glaucoma is a chronic disease resulting from damage and loss of retinal ganglion cells whose axons make up the optic nerve. The mechanism of this loss is unknown. While an increase in intraocular pressure is the hallmark risk factor, some have suggested the involvement of other factors. Such factors include inflammatory processes, oxidative stress, metabolic irregularities, or blood flow disturbances 56-58. In order to uncover the precise mechanism of cell death in this disease, researchers need simple, repeatable, and functional ways to accurately mimic conditions appearing in human glaucoma. Only then can researchers hope to devise a way to protect retinal ganglion cells from dying. The procedure described in this paper uses an artificially induced elevation of IOP to produce a gradual, irreversible loss of retinal ganglion cells similar to that seen in glaucoma patients 31. The procedure is minimally invasive. Significant retinal ganglion cell loss is measured within one month of surgery. This method is one significant tool for the study of glaucoma. A potential limitation of this method is the manual injection of hypertonic saline. Because of this manual method, it is possible to expect great variability in results. However, we have identified the blanching effect in the vein to be a critical step. If blanching occurs, retinal ganglion cell loss is always between 18 and 29%. To support this, all future studies could modify the procedure to include routine IOP measurements to ensure that these injections lead to a measurable increase in IOP. 29,31. Perhaps this model of RGC death will lead to the development of a more complete neuroprotective treatment that combats the devastating visual loss affecting millions of people worldwide.
Divulgazioni
The authors have nothing to disclose.
Acknowledgements
C. Linn is supported by an NIH grant (NIH NEI EY022795).
Materials
| Xylazine hydrochloride, Minimum 99% | Sigma, Life Science | X1251-1G | |
| Ketamine hydrochloride injection, USP, 100mg/mL | Putney, Inc | NDC 26637-411-01 | 10 mL bottle |
| Acepromazine Maleate, 10mg/mL | Phoenix Pharmaceutical, Inc | NDC 57319-447-04, 670008L-03-0408 | 50 mL bottle |
| Serum bottle, 10 mL | VWR | 16171319 | Borosilicate glass |
| 1 mL insulin syringe | VWR | BD329410 | 28 gauge needle |
| Sodium chloride | Sigma | S7653 | 2 M Solution |
| Microelectrode Puller | Narishige Group | PP-830 | |
| Heavy Polished Standard and Thin Walled Borosilicate Tubing | Sutter Instruments | B150-86-10HP | without filament, 0.86 mm |
| Microfil syringe needle for filling micropipettes | World Precision Instruments, Inc | MF28G | |
| 18 gauge Luer-Lock needle | Fisher Scientific | 1130421 | Syringe needle |
| Flexible Polyethylene Tubing | Fisher Scientific | 22046941 | 0.034 inch diameter, approximately 10 inches |
| Proparacaine Hydrochloride Opthalmic Solution, USP, 0.5% | Akorn, Inc | NDC 17478-263-12 | 15 mL sterile bottle |
| Curved Scissors | Fine Science Tools | 14061-11 | |
| Microscope | Leica | StereoZoom 4 | |
| Hemostat Clamp | Fine Science Tools | 1310912 | curved edge |
| Triple Antibiotic Ointment | Fisher Scientific | NC0664481 | |
| Scalpel handle | Fine Science Tools | 10004-13 | |
| Scalpel blade # 11 | Fine Science Tools | 10011-00 | |
| 60 mm x 15 mm Disposable Petri Dish | VWR | 351007 | |
| Phosphate Buffered Saline 10x Concentrate | Sigma, Life Science | P7059-1L | 1x dilution |
| Spring Scissors | Fine Science Tools | 15009-08 | |
| Forceps (2), Dumont # 5 | Fine Science Tools | 11251-30 | |
| 3 mL Transfer Pipets, polyethylene, non sterile | BD Biosciences | 357524 or 52947-948 | 1 and 2 mL graduations |
| 35 mm x 10 mm Easy Grip Petri Dish | BD Biosciences | 351008 | |
| Sylgard 184 | VWR | 102092-312 | |
| Cactus Needles | N/A | N/A | |
| Paraformaldehyde | EMD Millipore | PX0055-3 or 818715.0100 | Made into a 4% solution |
| Triton X-100 | Sigma | T9284-100 mL | Made into both a 1% and 0.1% solution |
| Fetal Bovine Serum | Atlanta Biological | S11150 | 500 ml |
| Purified Mouse Anti-Rat CD90/mouse CD90.1 | BD Pharmingen | Cat 554892 | 1:300 dilution |
| Alexa Fluor 594 goat anti-mouse | Life Technologies | A11005 | 1:300 dilution |
| Microscope Slides | Corning | 2948-75×25 | |
| Glycerol | Sigma | G5516-100 mL | 50% glycerol to 50% PBS, by weight |
| Coverglass | Corning | 2975-225 | Thickness 1 22 x 50 mm |
| Confocal Microscope | Nikon | C2 Eclipse Ti |
Riferimenti
- Goel, M., Picciani, R. G., Lee, R. K., Bhattacharya, S. K. Aqueous Humor Dynamics: A Review. Open Ophthalmol. J. 4, 52-59 (2010).
- Thylefors, B., Negrel, A. D. The global impact of glaucoma. Bull. World Health Organ. 72 (3), 323-326 (1994).
- Thylefors, B., Negrel, A. D., Pararajasegaram, R., Dadzie, K. Y. Global data on blindness. Bull. World Health Organ. 73 (1), 115-121 (1995).
- Roodhooft, J. M. Leading causes of blindness worldwide. Bull Soc. Belge. Ophtalmol. 283, 19-25 (2002).
- Sacca, S., Pulliero, A., Izzotti, A. The Dysfunction of the Trabecular Meshwork During Glaucoma Course. J. Cell. Physiol. 230 (3), 510-525 (2014).
- McKinnon, S. J., Goldberg, L. D., Peeple, P., Walt, J. G., Bramley, T. J. Current Management of Glaucoma and the Need for Complete Therapy. Am. J. Manag. Care. 14 (1 Suppl), S20-S27 (2008).
- Lee, D. A., Higginbotham, E. J. Glaucoma and its treatment: a review. Am. J. Health Syst. Pharm. 62, 691-699 (2005).
- Brandt, J. D., Vandenburgh, A. M., Chen, K., Whitcup, S. M. Bimatoprost Study Group. Comparison of once- or twice-daily bimatoprost with twice-daily timolol in patients with elevated IOP: a 3-month clinical trial. Ophthalmology. 108, 1023-1031 (2001).
- Camras, C. B. Comparison of latanoprost and timolol in patients with ocular hypertension and glaucoma: a six-month masked, multicenter trial in the United States. The United States Latanoprost Study Group. Ophthalmology. 103, 138-147 (1996).
- Netland, P. A., et al. Travoprost compared with latanoprost and timolol in patients with open-angle glaucoma or ocular hypertension. Am. J. Ophthalmol. 132, 472-484 (2001).
- Sherwood, M., Brandt, J. Bimatoprost Study Groups 1 and 2. Six-month comparison of bimatoprost once-daily and twice-daily with timolol twice-daily in patients with elevated intraocular pressure. Surv. Ophthalmol. 45 (Suppl 4), S361-S368 (2001).
- Watson, P., Stjernschantz, J. A six-month, randomized, double-masked study comparing latanoprost with timolol in open-angle glaucoma and ocular hypertension. The Latanoprost Study Group. Ophthalmology. 103, 126-137 (1996).
- Hedman, K., Alm, A., Gross, R. L. Pooled-data analysis of three randomized double-masked, six-month studies comparing intraocular pressure-reducing effects of latanoprost and timolol in patients with ocular hypertension. J. Glaucoma. 12 (6), 463-465 (2003).
- Schumer, R. A., Podos, S. M. The nerve of glaucoma!. Arch. Ophthalmol. 112, 37-44 (1994).
- Tsai, J. C., Chang, H. W. Comparison of the effects of brimonidine 0.2% and timolol 0.5% on retinal nerve fiber layer thickness in ocular hypertensive patients: a prospective, unmasked study. J. Ocul. Pharmacol. Ther. 21 (6), 475-482 (2005).
- Wilhelm, B., Ludtke, H., Wilhelm, H. The BRAION Study Group. Efficacy and tolerability of 0.2% brimonidine tartrate for the treatment of acute non-arteritic anterior ischemic optic neuropathy (NAION): a 3-month, double-masked, randomised, placebo-controlled trial. Graefes Arch. Clin. Exp. Ophthalmol. 244, 551-558 (2006).
- Fazzone, H. E., Kupersmith, M. J., Leibmann, J. Does topical brimonidine tartrate help NAION?. Br. J. Ophthalmol. 87, 1193-1194 (2003).
- Harris, A., Arend, O., Kagemann, L., Garrett, M., Chung, H. S., Martin, B. Dorzolamide, visual function and ocular hemodynamics in normal-tension glaucoma. J. Ocul. Pharmacol. Ther. 15, 189-197 (1999).
- Leahy, K. E., White, A. J. Selective laser trabeculoplasty: current perspectives. Clin. Ophthalmol. 11 (9), 833-841 (2015).
- Nesaratnam, N., Sarkies, N., Martin, K. R., Shahid, H. Pre-operative intraocular pressure does not influence outcome of trabeculectomy surgery: a retrospective cohort study. BMC Ophthalmol. 15 (1), 17 (2015).
- Cairns, J. E. Trabeculectomy. Preliminary report of a new method. Am. J. Ophthalmol. 66 (4), 673-679 (1968).
- Cheng, J. W., Cai, J. P., Wei, R. L. Meta-analysis of medical intervention for normal tension glaucoma. Ophthalomology. 116 (7), 1243-1249 (2009).
- Dielmans, I., Vingerling, J. R., Wolfs, R. C. W., Hofman, A., Grobbee, D. E., deJong, P. T. V. M. The prevalence of primary open-angle glaucoma in a population based study in The Netherlands: the Rotterdam Study. Ophthalmology. 101, 1851-1855 (1994).
- Lichter, P. R., et al. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology. 108 (11), 1943-1953 (2001).
- Heijl, A., et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 120 (10), 1268-1279 (2002).
- Kass, M. A., et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch. Ophthalmol. 120 (6), 701-713 (2002).
- Beidoe, G., Mousa, S. A. Current primary open-angle glaucoma treatments and future directions. Clin. Ophthalmol. 6, 1699-1707 (2012).
- Jeong, J. H., Park, K. H., Jeoung, J. W., Kim, D. M. Preperimetric normal tension glaucoma study: long-term clinical course and effect of therapeutic lowering of intraocular pressure. Acta. Ophthalmol. 92 (3), e185-e193 (2014).
- Morrison, J. C., Moore, C. G., Deppmeier, L. M., Gold, B. G., Meshul, C. K., Johnson, E. C. A Rat Model of Chronic Pressure-Induced Optic Nerve Damage. Exp. Eye Res. 64 (1), 85-96 (1997).
- Morrison, J. C., Johnson, E., Cepurna, W. O. Rat Models for Glaucoma Research. Prog. Brain Res. 173, 285-301 (2008).
- Iwamoto, K., Birkholz, P., Schipper, A., Mata, D., Linn, D. M., Linn, C. L. A Nicotinic Acetylcholine Receptor Agonist Prevents Loss of Retinal Ganglion Cells in a Glaucoma Model. Invest. Ophthalmol. Vis. Sci. 55 (2), 1078-1087 (2014).
- Morrison, J. C., Fraunfelder, F. W., Milne, S. T., Moore, C. G. Limbal Microvasculature of the Rat Eye. Invest. Ophthalmol. Vis. Sci. 36 (3), 751-756 (1995).
- McKinnon, S. J., Schlamp, C. L., Nickells, R. W. Mouse Models of Retinal Ganglion Cell Death and Glaucoma. Exp. Eye Res. 88 (4), 816-824 (2009).
- Maass, A., et al. Assessment of Rat and Mouse RGC Apoptosis Imaging in Vivo with Different Scanning Laser Ophthalmoscopes. Curr. Eye Res. 32 (10), 851-861 (2007).
- Li, Y., Schlamp, C. L., Nickells, R. W. Experimental induction of retinal ganglion cell death in adult mice. Investig. Ophthalmol. Vis. Sci. 40 (5), 1004-1008 (1999).
- Gross, R. L., et al. A mouse model of elevated intraocular pressure: retina and optic nerve findings. Trans. Am. Ophthalmol. Soc. 101, 163-171 (2003).
- Cenni, M. C., Bonfanti, L., Martinou, J. C., Ratto, G. M., Strettoi, E., Maffei, L. Long-term survival of retinal ganglion cells following optic nerve section in adult bcl-2 transgenic mice. Eur. J. Neurosci. 8 (8), 1735-1745 (1996).
- Templeton, J. P., Geisert, E. E. A practical approach to optic nerve crush in the mouse. Mol. Vis. 18, 2147-2152 (2012).
- Schlamp, C. L., Johnson, E. C., Li, Y., Morrison, J. C., Nickells, R. W. Changes in Thy1 gene expression associated with damaged retinal ganglion cells. Mol. Vis. 7, 192-201 (2001).
- Libby, R. T., et al. Susceptibility to neurodegeneration in a glaucoma is modified by Bax gene dosage. PLoS Genet. 1, 17-26 (2005).
- Yang, Z., et al. Changes in gene expression in experimental glaucoma and optic nerve transection: the equilibrium between protective and detrimental mechanisms. Invest. Ophthalmol. Vis. Sci. 48 (12), 5539-5548 (2007).
- Huang, W., Fileta, J., Guo, Y., Grosskreutz, C. L. Downregulation of Thy1 in retinal ganglion cells in experimental glaucoma. Curr. Eye Res. 31 (3), 265-271 (2006).
- Smedowski, A., Pietrucha-Dutczak, M., Kaarniranta, K., Lewin-Kowalik, J. A rat experimental model of glaucoma incorporating rapid-onset elevation of intraocular pressure. Sci. Rep. 4, 1-11 (2014).
- Cone, F. E., Gelman, S. E., Son, J. L., Pease, M. E., Quigley, H. A. Differential susceptibility to experimental glaucoma among 3 mouse strains using bead and viscoelastic injection. Exp. Eye Res. 91 (3), 415-424 (2010).
- Pease, M. E., Cone, F. E., Gelman, S., Son, J. L., Quigley, H. A. Calibration of the TonoLab tonometer in mice with spontaneous or experimental glaucoma. Invest. Ophthalmol. Vis. Sci. 52 (2), 858-864 (2011).
- Cone, F. E., et al. The effects of anesthesia, mouse strain and age on intraocular pressure and an improved murine model of experimental glaucoma. Exp. Eye Res. 99, 27-35 (2012).
- Frankfort, B. J., et al. Elevated intraocular pressure causes inner retinal dysfunction before cell loss in a mouse model of experimental glaucoma. Invest. Ophthalmol. Vis. Sci. 54 (1), 762-770 (2013).
- Sappington, R. M., Carlson, B. J., Crish, S. D., Calkins, D. J. The microbead occlusion model: a paradigm for induced ocular hypertension in rats and mice. Invest. Ophthalmol. Vis. Sci. 51 (1), 207-216 (2010).
- Kalesnykas, G., et al. Retinal ganglion cell morphology after optic nerve crush and experimental glaucoma. Invest. Ophthalmol. Vis. Sci. 53 (7), 3847-3857 (2012).
- Cone-Kimball, E., et al. Scleral structural alterations associated with chronic experimental intraocular pressure elevation in mice. Mol. Vis. 19, 2023-2039 (2013).
- Samsel, P. A., Kisiswa, L., Erichsen, J. T., Cross, S. D., Morgan, J. E. A novel method for the induction of experimental glaucoma using magnetic microspheres. Invest. Ophthalmol. Vis. Sci. 52 (3), 1671-1675 (2011).
- WoldeMussie, E., Ruiz, G., Wijono, M., Wheeler, L. A. Neuroprotection of retinal ganglion cells by brimonidine in rats with laser-induced chronic ocular hypertension. Invest. Ophthalmol. Vis. Sci. 42 (12), 2849-2855 (2001).
- Garcia-Valenzuela, E., Shareef, S., Walsh, J., Sharma, S. C. Programmed cell death of retinal ganglion cells during experimental glaucoma. Exp. Eye Res. 61 (1), 33-44 (1995).
- Aihara, M., Lindsey, J. D., Weinreb, R. N. Experimental mouse ocular hypertension: establishment of the model. Investig. Ophthalmol. Vis. Sci. 44 (10), 4314-4320 (2003).
- Ji, J., et al. Effects of elevated intraocular pressure on mouse retinal ganglion cells. Vision Res. 45 (2), 169-179 (2005).
- Flammer, J., et al. The eye and the heart. Eur. Heart J. 34 (17), 1270-1278 (2013).
- Gugleta, K., et al. Association between risk factors and glaucomatous damage in untreated primary open-angle glaucoma. J. Glaucoma. 22 (6), 501-505 (2013).
- Mozaffarieh, M., Flammer, J. New insights in the pathogenesis and treatment of normal tension glaucoma. Curr. Opin. Pharmacol. 13 (1), 43-49 (2013).
