The steps of the surgical procedure described in this protocol are summarized and illustrated in Figure 1. Briefly, prior to surgery, mice are anesthetized and the hair over the left thorax is removed. Mice are intubated and mechanically ventilated to enable survival upon breachment of the thoracic cavity. Soft tissue overlying the ribs is excised, and a small circular defect is created, spanning the 6th and 7th ribs. The optical window frame is inserted into the defect and its bottom side (outside of the clear aperture) is adhered to the lung tissue. The window frame is then secured with a combination of sutures and adhesive, resealing the thoracic cavity and permitting the resumption of normal breathing following extubation. When successfully implanted, the lung will adhere to the optical window (which is incorporated as part of the chest wall), with intrathoracic pressure gradients preserved. This permits comfortable survival of the mouse, enabling daily imaging up to the protocol allowance (2 weeks). Intravital imaging can then be performed through the window, as previously described for other windows15,19,20.
For visualization of various cell types, biological structures, or cellular functional states, the procedure presented here can be performed on a wide range of mice that have either been genetically manipulated to express fluorescent proteins21 or injected with dyes22. The permanent nature of the window makes it compatible with techniques for relocalization of fields of view such as photoconversion23,24 or microcartography17,18. Microcartography is a triangulation technique based upon using computed transformations of coordinates of fixed fiducial marks between imaging sessions in order to predict and re-localize a region of interest. In the window created as described above, these fiducial marks are light scratches etched into the window frame (Supplemental Figure 2) that are easily identifiable under the microscope. This makes it possible to find the same field of view multiple times, even in otherwise unmarked tissue. Figure 2 demonstrates the result of these techniques in a mouse where the lung vasculature has been labeled by injection of a dye-labeled high molecular weight dextran (tetramethylrhodamine 155 kD dextran) and the same micro-vasculature re-localized over 3 days.
This dextran was found to be extremely useful in evaluating transient vascular openings that are induced during periods of tumor cell intravasation25,26,27. Indeed, it has been shown that, in primary breast tumors, this high molecular weight dextran is otherwise effectively sequestered to the vasculature and does not leak into the interstitium25. This is in contrast to dextrans of lower molecular weight (such as 10 kD or 70 kD), which have been shown to leak from neoangiogenic vessels passively28,29. Meanwhile, the healthy lung vasculature has been observed to be more resistant to leakage, with dextrans >10 kD only escaping to the interstitium upon insult to the organ, such as upon exposure to exosomes30 or viruses31. A variety of contrast agents also exist to measure other parameters in the lung (e.g., nuclear markers, live/dead indicators, oxidative stress reporters, blood flow velocity trackers) in addition to vascular permeability. An excellent resource cataloging them can be found in the protocol by Ueki et al.22.
The WHRIL is a technique that is very well-suited to investigating the dynamics of blood flow in the lung. This can be accomplished in several ways. First, when imaged using relatively slow frame rates (~1-10 frames per second, fps) blood flow velocities can be determined by the shadows that unlabeled erythrocytes make when flowing in larger vessels. At low fps, these shadows form lines whose angle relative to the vessel can be used to calculate erythrocyte flow rates32 (Figure 2, yellow lines). Second, shadows can also be tracked on low fps microscopes by aligning the vessels with the fast scan axis of the microscope and acquiring kymographs using rapid line scanning33,34,35. Finally, when imaging at high frame rates (>10 fps) on a microscope capable of integrating the signal over time (e.g., a spinning disk confocal equipped with a charge-coupled device (CCD) detector), individual particles can be traced directly16,17. In this situation, stationary objects appear as bright dots, and flowing objects trace out tracks through with the circulation. Cell speeds can be quantified by measuring the length of the tracks and dividing by the frame acquisition time. An example of this is given in Figure 3 and Supplemental Movie 1, where 2 µm fluorescent microspheres have been intravascularly injected into the mouse before imaging.
With the ability to repeatedly and consistently return to the same field of view, visualization of processes that evolve over multiple days is now possible. As a demonstration of this application, the WHRIL was used to visualize the metastatic progression of breast cancer cells within the lungs17,21: that is, to track over time the fate of individual tumor cells that arrive at the lung vasculature. This concept is depicted in Figure 4A, where a single disseminated tumor cell is visualized shortly after lodging in a segment of lung micro-vasculature. Returning to that same location on subsequent days reveals the tumor cell's fate (e.g., recirculation, extravasation, etc.). Applied to the investigation of the culminating steps of metastatic progression in the lung, it was possible to visually chronicle dynamic processes, including tumor cell arrival (Figure 4B), extravasation (Figure 4C), and proliferation to form macro-metastasis (Figure 4D).
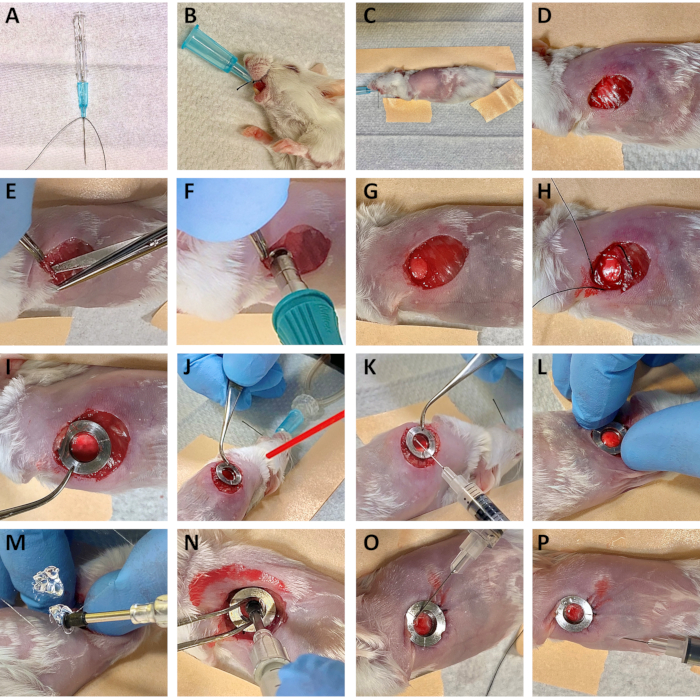
Figure 1: Summary of surgery for the implantation of the Window for High-Resolution Imaging of the Lung (WHRIL). Please click here to view a larger version of this figure.
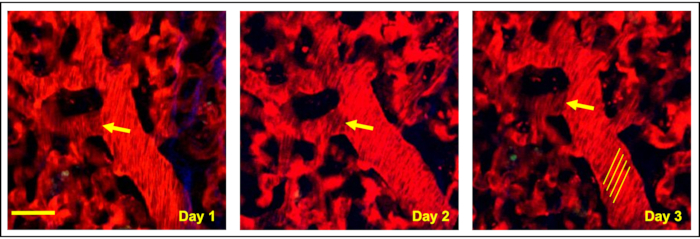
Figure 2: Microcartography enables the relocalization of fixed positions within the optical window. Multiphoton intravital imaging of a single region of the lung under the optically transparent coverslip shows microvasculature relocated over 3 consecutive days using microcartography. Yellow arrows indicate a clearly definable branch point from a single vessel identified each consecutive day. Yellow lines highlight shadows that unlabeled erythrocytes make when flowing in larger vessels. The angle of these lines relative to the vessel can be used to calculate erythrocyte flow rates. Red = tdTomato labeled endothelial cells and 155 kDa Tetramethylrhodamine dextran labeled blood serum, Green = GFP labeled tumor cells, Blue = second harmonic generation. Scale bar = 15 µm. Please click here to view a larger version of this figure.
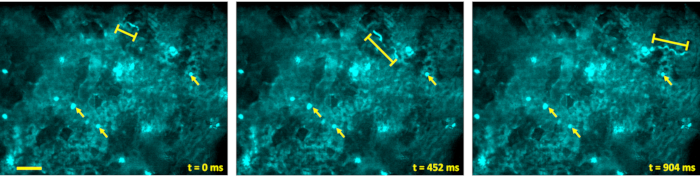
Figure 3: Visualization of blood flow rate. Blood flow rates can be visualized by injecting 2 µm diameter fluorescent microspheres retro-orbitally and imaging their passage through the blood vessels. When imaged on a microscope capable of integrating the signal over time (e.g., a spinning disk confocal equipped with a CCD detector), stationary microspheres appear as bright dots (arrows), and flowing spheres trace out tracks through with the circulation (bracketed lines). Scale bar = 50 µm. Please click here to view a larger version of this figure.
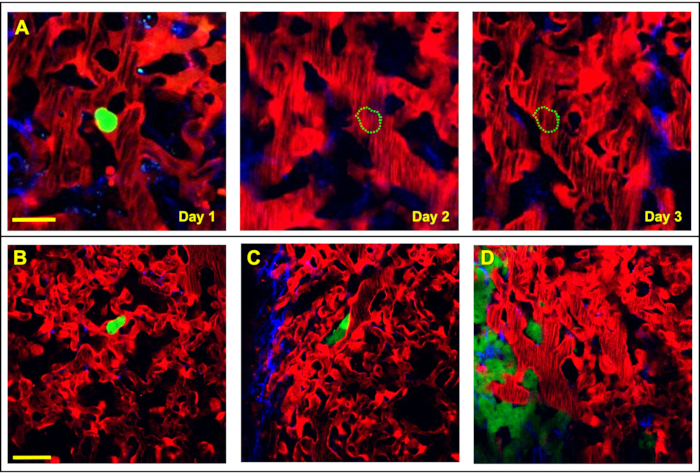
Figure 4. The WHRIL can capture each step of the metastatic cascade within the lung by directly visualizing the fate of disseminated tumor cells. (A) Tracking the fate of disseminated tumor cells (green) is achievable with serial imaging, over several days, through the WHRIL. On Day 1, a tumor cell is observed to have arrived to and lodged in the lung vasculature. On Day 2 and Day 3 the cell is no longer present in the lung vasculature, having either recirculated or died. Scale bar = 15 µm. (B–D) Visualization of each of the stages of tumor cell metastasis in the lung. (B) An intravascular disseminated tumor cell (green) lodged in the lung vasculature after arrival. (C) Disseminated tumor cell (green) after extravasating into the lung parenchyma. (D) Tumor cells that have proliferated and grown into micro-metastases. Red = tdTomato labeled endothelial cells and 155 kDa Tetramethylrhodamine dextran labeled blood serum, Green = GFP labeled tumor cells, Blue = second harmonic generation. Scale bar = 20 µm. Please click here to view a larger version of this figure.
Supplemental Movie 1: Video corresponding to Figure 3 showing the lung vasculature with circulating 2 µm microspheres. Please click here to download this Movie.
Supplemental Figure 1: Mechanical design drawings for the stainless-steel cutting tool used to guide the 5 mm biopsy punch. Please click here to download this File.
Supplemental Figure 2: Mechanical design drawings for the stainless-steel window frame. Please click here to download this File.
Supplemental Figure 3: Mechanical design drawings for the window holder tool. Please click here to download this File.
