ويقدر أن نصف سكان الولايات المتحدة يعاني من كسر في سن 65 1. بالنسبة لأولئك المرضى الذين يعانون من كسور المعالجة جراحيا، تشمل 500،000 إجراءات استخدام الكسب غير المشروع العظام 2 و من المتوقع أن يرتفع مع شيخوخة السكان على نحو متزايد 3 هذا العدد . على الرغم من أن العظام هي واحدة من عدد قليل من الأجهزة التي لديها القدرة على شفاء تماما بدون تندب، هناك حالات حيث فشل عملية 3،4. تبعا للظروف ونوعية العلاج، 2-30٪ من كسور العظام الطويلة تفشل، مما أدى إلى عدم النقابات 3،5. في حين لا يزال هناك بعض الجدل حول تعريف، فصال كاذب، وإصابات حرجة الحجم أو غير نقابية العظام تشير بصفة عامة إلى إصابة لا يلتئم على مدى عمر الطبيعي لهذا الموضوع (6). لأغراض تجريبية، هو تقصير هذه المدة إلى متوسط الوقت اللازم للشفاء التام من متوسط الحجم إصابة العظام. تحدث الآفات العظام غير نقابية لالأسطواناتأسباب erous، ولكن العوامل الرئيسية وتشمل الصدمة الشديدة مما أدى إلى وجود فجوة خطيرة الحجم، والعدوى، وضعف الأوعية الدموية، واستخدام التبغ، أو قدرة osteoregenerative تحول دون ذلك بسبب المرض أو العمر 7. حتى لو يتم التعامل غير النقابات بنجاح، فإنه يمكن أن تكلف ما يزيد على 60،000 دولار في الإجراء، وهذا يتوقف على نوع الإصابة والمناهج المستخدمة 8.
وفي الحالات المعتدلة، وتوظيف ذاتي ترقيع العظام. وتتضمن هذه الاستراتيجية استرداد العظام من موقع المانحة وغرس في موقع الإصابة. في حين أن هذا النهج هو فعالة للغاية، وحجم متاح العظام المستمدة المانحة محدود وينطوي على إجراء عملية جراحية إضافية، مما يؤدي إلى ألم مستمر في العديد من المرضى 9،10. وبالإضافة إلى ذلك، فإن فعالية من الكسب غير المشروع العظام ذاتي يعتمد على صحة المريض. هي بدائل العظام مصنوعة من مواد تركيبية أو معالجتها العظام جثي متوافرة بكثرة 11-13، لكنها هكتارلقد قيود كبيرة، بما في ذلك سوء خصائص التصاق الخلية المضيفة، وانخفاض osteoconductivity، وإمكانية الرفض المناعي 14. ولذلك هناك حاجة ملحة لتقنيات تجديد العظام التي هي آمنة وفعالة ومتاحة على نطاق واسع.
لدينا القدرة على تحسين استراتيجيات التجدد العظام تعتمد بشكل كبير على القدرة على تقليد الصدمة العظام خطيرة في حيوانات التجارب، ولكن الجيل واستقرار الآفات العظام كبيرة يمثل تحديا تقنيا. في معظم الحالات، يتم تحاكي صدمة خطيرة العظام الطويلة تجريبيا من خلال إنشاء الخلل التي لن تلتئم بشكل طبيعي. على الرغم من أنه يمكن أن تختلف مع الأنواع 15، ويتحقق ذلك عن طريق الإزالة الكاملة للشريحة العظام أكبر من 1.5 مرة من قطر العظام المقطع العرضي 16. ثم يستقر العظام مع زرع المعادن للحفاظ على التوجه السليم من حواف كسر والسماح للتنقل. نظرا لصغر حجمها وهشاشةالعظام الطويلة، وإنشاء مثل هذه الآفات في الفئران هم أبعد من قدرات معظم المجموعات البحثية. على هذا النحو، تقتصر نماذج عيب العظام الطويلة للفئران والحيوانات الكبيرة. ومع ذلك، والفئران تحمل مزايا البحثية الهامة في أنها يمكن المعدلة وراثيا وتربيتها كما سلالات خطر المناعية التي لا نرفض الخلايا البشرية والأنسجة.
لالتطبيقات المستندة إلى خلية الإنسان والفئران خطر المناعية جذابة للعمل مع لأنها من الناحية الفسيولوجية تتميز بشكل جيد، وسهلة المنزل، وفعالة من حيث التكلفة، وسهولة تحليلها شعاعيا وتشريحيا. من الأهمية بمكان أن الفئران خطر المناعية لا يرفض الخلايا من مختلف الأنواع بما في ذلك البشر. يسمح صغر حجمها أيضا اختبار أعداد صغيرة جدا من الخلايا أو مجلدات من السقالات التجريبية في تطبيقات العظام. تم الإبلاغ عن عدة نماذج تقويم العظام الفئران التي تحمل درجات مختلفة من الاستقرار العظام 17،18. تلك التنفسيمللي التي تؤدي إلى مستويات عالية جدا من الاستقرار، مثل المثبتات الخارجية وتأمين لوحات تلتئم في الغالب من قبل التحجر داخل الغشاء على الرغم من أن الشفاء غضروفي وقد تم الإبلاغ عن 19. في المقابل، تلك التي تسمح بعض المتناهية الصغر و / أو الحركة الماكرو، مثل تلك التي تستخدم المسامير النخاعية غير المثبتة أو جزئيا ثابتة، وشفاء بشكل عام مع غلبة التحجر غضروفي 20،21. اتحاد تأخر أو عيوب غير نقابية من العظام الطويلة من الصعب بشكل خاص لتحقيق في الفئران بسبب مستوى إضافي من الاستقرار المطلوب. ومع ذلك، فقد تم الإبلاغ عن عدد من النهج، بما في ذلك دبابيس النخاعية مع المسامير المتشابكة، وتأمين لوحات والمثبتات الخارجية 22. هذه الأنظمة تعمل بشكل جيد عموما، ولكن نظرا تصميم معقد من أنها يمكن أن يكون تحديا تقنيا لتثبيت. على سبيل المثال، جارسيا وآخرون. 23 وضعت على المتشابكة نظام دبوس أنيق للاستخدام في الفئران، ولكن ينطوي على إجراء شقوق في اثنين الموقع مستقلالصورة وتعديل واسع من عظم الفخذ لاستيعاب الدبابيس. وأجريت هذه الإجراءات تحت المجهر تشريح.
هنا، نحن تصف دبوس النخاع الفخذ بسيط مع طوق المركزي تهدف إلى منع إغلاق عجز العظم 3 مم وكذلك ترسيم حواف الأصلية للعيب. في حين دبوس لم يحدد حتى العظم نفسه، وتحجيم دقيق لقطر دبوس والتوسيع من نتائج تجويف النخاع في التدخل كافية للحد من الحركة الالتوائية (الشكل 1). مع اختيار دقيق من العمر الفطرية ونوع الجنس والفئران المتطابقة سلالة، والنتيجة هي تكرار للغاية التصنع غير uniondefect-22 التي يمكن تقييمها بسهولة شعاعيا. وعلاوة على ذلك المناطق ذات الاهتمام يمكن تعريف بتكاثر بعد التصوير المقطعي-حسابها الصغرى (μCT) لقياس دي نوفو تكوين العظام والمعلمات histomorphological. تم نموذج أولي من المسامير في مختبرنا باستخدام أدوات متوفرة بسهولة.
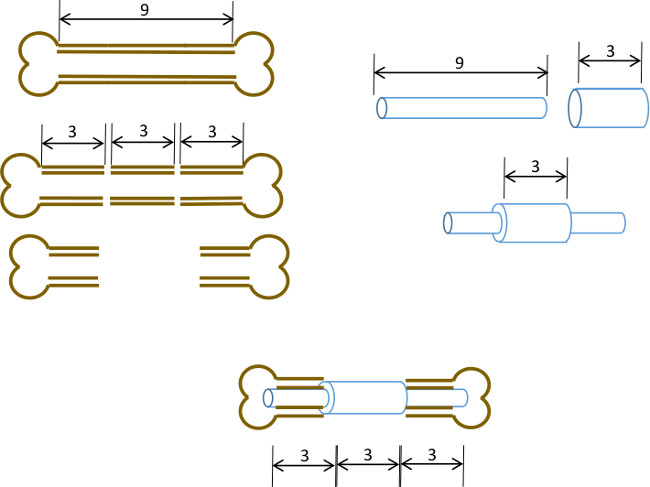
الشكل 1: مبدأ التجريبي ملخص بياني للنموذج الخلل القطعي. يتم استئصاله وسط شريحة 3 ملم من 9-10 ملم عظم الفخذ الفئران جراحيا (يسار). يتم تمرير 3 مم طويل، 19 مقياس أنابيب الصلب الجراحية أكثر من 9 ملم طويلة، 22 G أنبوب الفولاذ المقاوم للصدأ وثابتة بمادة لاصقة في وسط الدقيق (يمين). تم تجهيز دبوس الناتجة في القنوات النخاعية ما تبقى من أجزاء القريبة والبعيدة للعظم الفخذ مع G طوق 19 استبدال جزء 3 ملم من العظم (أدناه، وسط).
