הערכה היא כי מחצית מאוכלוסיית ארה"ב חווה שבר בגיל 65 1. עבור אותם מטופלים עם שברים שטופלו בניתוח, 500,000 הליכים כרוכים בשימוש בשתל עצם 2 ומספר זה צפוי לעלות עם הזדקנות אוכלוסייה יותר ויותר 3 . למרות שעצם הוא אחד מכמה איברים שיש את היכולת לרפא לחלוטין ללא צלקות, יש מקרים שבם התהליך נכשל 3,4. בהתאם לנסיבות ולאיכות טיפול, 2-30% משברים בעצמות ארוכות ייכשלו, וכתוצאה מכך 3,5 שאינו איגוד. אמנם יש עדיין ויכוח על ההגדרה, pseudoarthrosis, פציעות עצם הקריטיות בגודל או אי-איחוד בדרך כלל מתייחס לפגיעה שאינה נרפא במשך החיים הטבעיים של הנושא 6. למטרות ניסוי, משך זה מתקצר לזמן הממוצע שנדרש להחלמה של פציעה עצם בגודל ממוצעת מלאה. נגעי עצם ללא איחוד להתרחש numסיבות erous, אך גורמים עיקריים כוללות טראומה קיצונית וכתוצאה מכך פער קריטי בגודל, זיהום, אנגיוגנזה עניה, שימוש בטבק, או יכולת osteoregenerative עכבות עקב מחלה או גיל 7. גם אם מטופלים אינם איגודים בהצלחה, זה יכול לעלות בעודף של 60,000 $ להליך, בהתאם לסוג פציעה והגישות המועסקות 8.
במקרים מתונים, השתלת עצם אוטולוגית מועסקת. אסטרטגיה זו כרוכה בהחלמה של עצם מאתר תורם והשתלה באתר של פציעה. בעוד גישה זו היא מאוד יעילה, הנפח של עצם תורם נגזרות זמין מוגבל וההליך כרוך ניתוח נוסף, שתוצאתו כאב מתמשך בחולים רבים 9,10. בנוסף, היעילות של שתל עצם אוטולוגית תלויה של בריאותו של המטופל. תחליפי עצם עשויים מחומרים סינטטיים או עצם מגופות מעובד זמינים 11-13 בשפע, אבל הם חהve מגבלות משמעותיות, כוללים נכסים עניים הידבקות מארח תאים, osteoconductivity המופחת, והפוטנציאל לדחייה חיסונית 14. אין אפוא צורך דחוף בטכנולוגיות התחדשות עצם שבטוחות, יעילים וזמינות לציבור רחב.
היכולת שלנו לשפר את אסטרטגיות משובי עצם תלויה באופן קריטי על היכולת לחקות טראומת עצם חמורה בבעלי חיים בדיקה, אבל הדור והייצוב של נגעי עצם גדולים הוא מאתגר מבחינה טכנית. ברוב המקרים, טראומת עצם ארוך רצינית חיקתה בניסוי על ידי הקמת פגם שלא באופן טבעי לרפא. למרות שזה יכול להשתנות עם מינים 15, זו מושגת על ידי הסרת קטע עצם שהוא גדול יותר מ -1.5 פעמים הקוטר של עצם החתך 16 מלאה. העצם מכן התייצב עם שתל מתכת כדי לשמור על כיוון נכון של קצות שבר ולאפשר לניידות. בשל גודלם הקטן והשברירי שלהעצמות הארוכות שלהם, הקמת כזה נגעים בעכברים הן מעבר ליכולות של רוב קבוצות מחקר. ככזה, מודלים פגם עצם ארוך מוגבלים לחולדות ובעלי חיים גדולים יותר. עם זאת, עכברים יעניקו יתרונות משמעותיים במחקר שהם יכולים להיות מהונדסים גנטיים וגדלו כזנים שנפרץ חיסון שלא לדחות תאים ורקמות אנושיים.
עבור יישומים מבוססי תאים אנושיים, עכברים שנפרץ חיסון הם אטרקטיביים לעבוד איתו כי הם מבחינה פיזיולוגית מאופיינים היטב, קל לבית, חסכוני, בקלות ובנתח radiologically והיסטולוגיה. חשיבות עליונה הוא שעכברים שנפרץ חיסון לא דוחים תאים ממינים שונים כולל בני אדם. גודלם הקטן מאפשר גם הבדיקה של מספרים קטנים מאוד של תאים או כרכים של פיגומים ניסיוניים ביישומים אורטופדיים. כמה מודלים עכבריים אורתופדים כבר דיווחו כי להרשות לעצמו דרגות שונות של יציבות עצם 17,18. תוכנה לאלהms המוביל לרמות גבוהות מאוד של יציבות, כגון תופסנים חיצוניים וצלחות נעילה בעיקר לרפא על ידי התאבנות intramembranous למרות ריפוי endochondral דווח 19. בניגוד לכך, אלה המאפשרים כמה מיקרו ו / או מקרו-תנועה, כגון אלה המעסיקים סיכות לשדיות מבולבלות או חלקי-קבועות, בדרך כלל לרפא עם דומיננטיות של התאבנות endochondral 20,21. איגוד מושהה או פגמים שאינם איחוד של עצם ארוך הם קשה במיוחד להשגה בעכברים עקב הרמה נוספת של ייצוב הנדרשת. עם זאת, מספר גישות כבר דיווחו, כולל סיכות לשדיות עם ציפורני לובים, צלחות נעילה ותופסנים חיצוניים 22. מערכות אלה בדרך כלל עובדים היטב, אבל בהתחשב בעיצוב המסובך שלהם הם יכולים להיות מאתגרים מבחינה טכנית להתקנה. לדוגמא, גרסיה et al. 23 המציא מערכת סיכה שלובים אלגנטית לשימוש בעכברים, אבל ההליך כרוך חתכים בשני אתר נפרדים ושינוי נרחב של עצם הירך כדי להכיל את הסיכות. נהלים אלה בוצעו תחת מיקרוסקופ לנתח.
במסמך זה, אנו מתארים סיכה לשדית הירך פשוטה עם צווארון מרכזי שנועד למנוע סגירת גירעון עצם 3 מ"מ וגם להתוות את הקצוות המקוריים של הפגם. בעוד הסיכה לא הייתה קבועה לעצם עצמו, לשינוי גודל מדויק של קוטר הסיכה וreaming של תוצאות החלל הלשדיות בהתערבות מספיקה כדי למזער תנועת torsional (איור 1). עם בחירה זהירה של גיל טהור, מגדר ועכברים בהתאמה מתח, התוצאה היא שאינו uniondefect hypertrophic מאוד לשחזור 22 ניתן יהיה להעריך בקלות radiologically. יתר על כן אזורים של עניין יכולים להיות מוגדרים reproducibly לאחר טומוגרפיה-מחושב מיקרו (μCT) למדידת דה נובו היווצרות עצם ופרמטרי histomorphological. הסיכות היו prototyped במעבדה שלנו תוך שימוש בכלים זמינים.
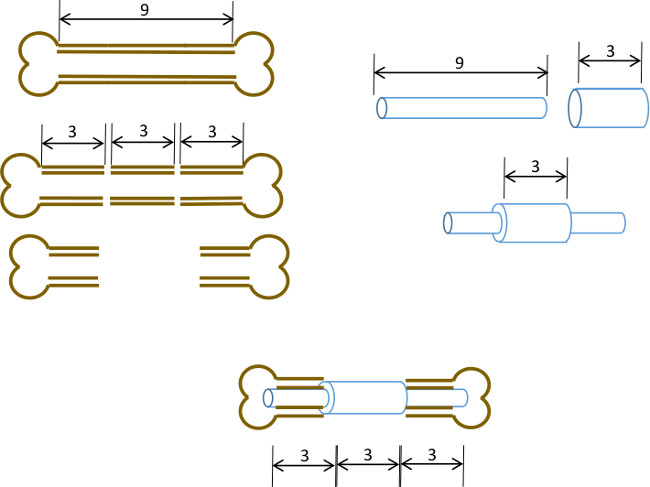
איור 1: עיקרון ניסויי סיכום תרשים של מודל הפגם המגזרי.. קטע 3 מ"מ המרכזי של עצם ירך עכברית 9-10 מ"מ הוא נכרת בניתוח (משמאל). צינור פלדה כירורגית ארוך 3 מ"מ, 19 מד הוא חלף על פני מ"מ ארוך 9, 22 צינור הנירוסטה G וקבוע עם דבק במרכז המדויק (מימין). סיכת התוצאה היא מצויד לתוך התעלות הלשדיות של החלקים הפרוקסימלית ודיסטלי הנותרים של עצם הירך עם 19 צווארון G החלפת קטע 3 מ"מ של עצם (להלן, במרכז).
