これは、治療骨折を有する患者のために外科的に50万手続きは骨移植片2の使用を含む。米国の人口の半分は65 1歳までに骨折を経験していると推定されており、この数は、ますます高齢化、人口3に上昇すると予想されている。骨が完全に瘢痕なしに治癒する能力を有するいくつかの臓器の一つであるが、プロセスは3,4失敗する場合がある。状況や処理の品質に応じて、長骨骨折の2〜30%は、非組合3,5で得られた、失敗。定義、偽関節、大きさのクリティカルまたは非組合骨損傷上のいくつかの議論が残っているものの、一般的に被検体6の自然な寿命にわたって治癒しない怪我を指します。実験目的のために、この期間は、平均的なサイズの骨損傷の完全な治癒に必要な平均時間に短縮される。非組合骨病変はNUMのために起こるerousの理由が、主な要因は、原因疾患や年齢7に批判的にサイズのギャップ、感染、貧しい血管新生、タバコの使用、または阻害osteoregenerative容量になり、極端な外傷が含まれる。非組合が正常に処理されたとしても、それは損傷の種類と8を採用アプローチに応じて、手順6万ドルを超える費用がかかる。
中程度の場合には、自家骨髄移植が用いられる。この戦略は、損傷部位でのドナー部位および移植から骨の回復を伴う。このアプローチは非常に有効であるが、利用可能なドナー由来の骨の量は限られており、手順は、多くの患者9,10において持続性疼痛をもたらす追加の手術を伴う。また、自家骨移植片の有効性は、患者の健康状態に依存する。合成材料または処理死体の骨から作られた代用骨は11-13豊富に利用可能ですが、彼 らはヘクタール乏しい宿主細胞の接着性、骨伝導性減少、および免疫拒絶14の可能性を含め、重大な制限VEの。安全で、効果的であり、広く利用可能な骨再生技術が緊急に必要とされている。
骨再生の戦略を改善する当社の能力は、試験動物に深刻な骨の外傷を模倣する能力に決定的に依存しているが、大きな骨病変の発生と安定化は技術的に困難である。ほとんどの場合、深刻な長骨の外傷が自然治癒しない欠陥を確立することによって実験的に模倣される。それは種15によって変化し得るが、これは骨の断面16の直径の1.5倍よりも大きい骨セグメントを完全に除去することによって達成される。骨は、その後骨折エッジの適切な配向を維持し、移動性を可能にするために、金属インプラントで安定化される。その小さなサイズとの脆弱性に起因する彼らの長い骨は、マウスではそのような病変の確立が最も研究グループの能力を超えている。このように、長骨欠損モデルは、ラットおよび大型動物に限定される。それにもかかわらず、マウスは、それらが遺伝的に修飾されたヒト細胞および組織を拒絶しない、免疫不全株として育種することができるという点で、重要な研究の利点をもたらす。
彼らは生理的によく特徴付けているため、ヒト細胞ベースのアプリケーションでは、免疫不全マウスはで動作するように魅力的で、家に簡単に、効果的なコスト、簡単に放射線学的および組織学的に分析した。最も重要な免疫不全マウスは、ヒトを含む異なる種からの細胞を拒絶しないことである。その小さなサイズはまた、細胞または整形外科用途で実験的な足場の体積の非常に少数のテストを可能にします。いくつかのマウスモデルが整形外科用骨安定17,18の様々な程度を与えることが報告されている。これらのsyste軟骨内の治癒が19に報告されているが、外部固定器とロッキングプレートとしての安定性の非常に高いレベルをもたらすmsが主に膜内骨化によって治癒する。対照的に、未修正または部分的に固定された髄ピンを用いたものなど、いくつかのミクロおよび/ またはマクロ運動を可能にするものは、一般的に軟骨内骨化20,21が優勢で治癒する。長骨の遅延組合や非組合欠陥が必要な安定化の余分なレベルに起因したマウスで達成することが特に困難である。しかし、多くのアプローチが、プレートと外部固定器22をロックする、インターロック爪と髄ピンを含む、報告されている。これらのシステムは、一般的にはうまく動作しますが、その複雑な設計与えられた彼らは、インストールすることが技術的に挑戦することができます。例えば、ガルシアら 23は、マウスにおける使用のための優雅なインターロックピン方式を考案したが、手順は、2つの別々の部位における切開を伴いピンを収容するための大腿骨の広範な修正。これらの手順は、解剖顕微鏡下で行った。
ここで、我々は、3ミリメートルの骨欠損の閉鎖を防止し、また、欠陥のオリジナルのエッジを描くように設計され、中央襟付きのシンプルな大腿骨髄ピンについて説明します。ピンは、骨自体に固定されなかったが、十分な干渉髄腔結果のピン径、およびリーマの正確なサイジングがねじれ運動( 図1)を最小化する。近交系、年齢、性別及び歪みを一致させたマウスを慎重に選択すると、結果は簡単に放射線学的に評価することが可能で再現性の高い肥大非uniondefect 22です。また、関心領域は、再現デノボ骨形成および組織形態学的パラメータを測定するためのマイクロコンピュータ断層撮影(μCT)の後に定義することができる。ピンは、容易に入手可能なツールを使用して、我々の研究室で試作された。
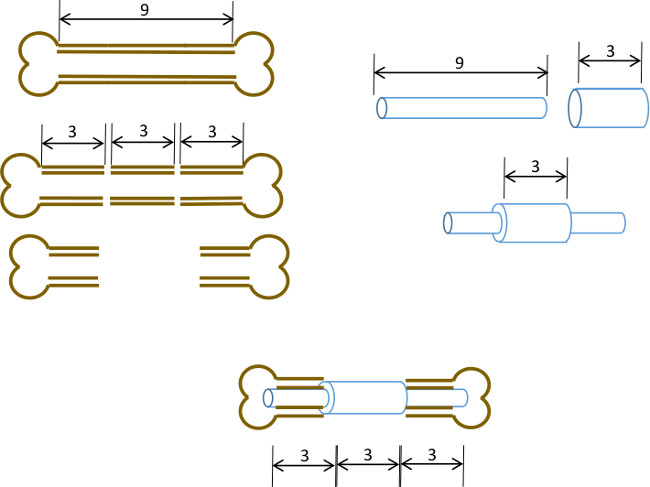
図1:実験原理分節欠損モデルの図的要約。 9〜10ミリメートルマウス大腿骨の中央の3ミリメートルのセグメントは、( 左 )外科的に切除されている。長さ3mm、19ゲージの外科用鋼管は、正確な中心( 右 )での長い9ミリメートル、22 Gステンレス管の上を通過し、接着剤で固定されている。得られたピンは、骨の3mmのセグメントを置き換える19 Gのカラー( 以下、センター )と大腿骨の残りの近位および遠位部分の髄運河に嵌め込まれている。
