यह इलाज भंग के साथ उन रोगियों के लिए शल्य चिकित्सा, 500,000 प्रक्रियाओं बोन ग्राफ्ट 2 का उपयोग शामिल है। अमेरिका की आबादी का आधा 65 1 साल की उम्र से एक फ्रैक्चर का अनुभव है कि अनुमान है और इस संख्या में एक तेजी से उम्र बढ़ने की आबादी 3 के साथ वृद्धि की उम्मीद है । हड्डी पूरी तरह से scarring के बिना चंगा करने के लिए क्षमता है कि कुछ अंगों में से एक है हालांकि प्रक्रिया 3,4 विफल रहता है, जहां उदाहरण हैं। हालात और इलाज की गुणवत्ता पर निर्भर करता है, लंबे समय से अस्थि भंग का 2-30% गैर संघ 3,5, जिसके परिणामस्वरूप में असफल। परिभाषा, pseudoarthrosis, आकार-महत्वपूर्ण या गैर संघ की हड्डी की चोटों पर कुछ बहस बनी हुई है जबकि आम तौर पर इस विषय 6 के प्राकृतिक जीवनकाल में ठीक नहीं है कि एक चोट को दर्शाता है। प्रयोगात्मक प्रयोजनों के लिए, इस अवधि के एक औसत आकार की हड्डी की चोट का पूर्ण उपचार के लिए आवश्यक औसत समय के लिए छोटा है। गैर संघ हड्डी घावों NUM के लिए होते हैंerous कारणों से है, लेकिन प्रमुख कारकों की वजह से बीमारी या 7 साल की उम्र के लिए एक गंभीर रूप से आकार की खाई, संक्रमण, गरीब एंजियोजिनेसिस, तंबाकू के इस्तेमाल, या हिचकते osteoregenerative क्षमता में जिसके परिणामस्वरूप चरम आघात शामिल हैं। गैर यूनियनों सफलतापूर्वक इलाज कर रहे हैं, भले ही यह चोट के प्रकार और 8 कार्यरत दृष्टिकोण पर निर्भर करता है, प्रक्रिया के अनुसार 60,000 डॉलर की अतिरिक्त में खर्च कर सकते हैं।
उदारवादी मामलों में, ऑटोलॉगस बोन ग्राफ्टिंग कार्यरत है। इस रणनीति के चोट के स्थल पर एक दाता साइट और आरोपण से हड्डी की वसूली शामिल है। इस दृष्टिकोण अत्यंत प्रभावी है, उपलब्ध दाता व्युत्पन्न हड्डी की मात्रा सीमित है और प्रक्रिया कई रोगियों 9,10 में लगातार दर्द में जो परिणाम एक अतिरिक्त सर्जरी, शामिल है। इसके अलावा, ऑटोलॉगस बोन ग्राफ्ट की प्रभावकारिता रोगी के स्वास्थ्य निर्भर है। सिंथेटिक सामग्री या संसाधित शव हड्डी से बना अस्थि के विकल्प 11-13 बहुतायत से उपलब्ध हैं, लेकिन वे हागरीब मेजबान कोशिका आसंजन गुण, कम osteoconductivity, और प्रतिरक्षा अस्वीकृति 14 के लिए संभावित सहित महत्वपूर्ण सीमाओं, ve। सुरक्षित, प्रभावी और व्यापक रूप से उपलब्ध हैं कि हड्डी पुनर्जनन प्रौद्योगिकियों के लिए एक तत्काल आवश्यकता इसलिए नहीं है।
हड्डी पुनर्योजी रणनीतियों में सुधार करने की क्षमता का परीक्षण पशुओं में गंभीर हड्डी आघात नकल करने की क्षमता पर निर्भर है, लेकिन बड़े हड्डी घावों की पीढ़ी और स्थिरीकरण तकनीकी रूप से चुनौती दे रहा है। ज्यादातर मामलों में, गंभीर लंबी हड्डी आघात स्वाभाविक रूप से ठीक नहीं होगा कि एक दोष की स्थापना के द्वारा प्रयोगात्मक मजाक उड़ाया जाता है। यह प्रजाति 15 के साथ अलग-अलग हो सकता है, यह हड्डी पार अनुभाग 16 के बड़े से 1.5 गुना व्यास है कि एक हड्डी खंड के पूरी तरह हटाने के द्वारा हासिल की है। हड्डी तो फ्रैक्चर किनारों की उचित उन्मुखीकरण को बनाए रखने और गतिशीलता के लिए अनुमति देने के लिए एक धातु प्रत्यारोपण के साथ स्थिर है। कारण उनके छोटे आकार और की कमजोरी कोउनकी लंबी हड्डियों, चूहों में इस तरह के घावों की स्थापना के सबसे अनुसंधान समूहों की क्षमताओं से परे हैं। जैसे, लंबी हड्डी दोष मॉडल चूहों और बड़े जानवरों तक ही सीमित हैं। फिर भी, चूहों वे आनुवंशिक रूप से संशोधित और मानव कोशिकाओं और ऊतकों को अस्वीकार नहीं करते कि प्रतिरक्षा समझौता किया उपभेदों के रूप में पैदा किया जा सकता है कि में महत्वपूर्ण अनुसंधान फायदे बनती हैं।
मानव कोशिका आधारित अनुप्रयोगों के लिए, प्रतिरक्षा-समझौता किया चूहों वे physiologically घर के लिए आसान है, अच्छी तरह से विशेषता हैं क्योंकि के साथ काम करने के लिए आकर्षक हैं, लागत प्रभावी, और आसानी से histologically radiologically और विश्लेषण किया। सर्वोच्च महत्व का प्रतिरक्षा समझौता किया चूहों मानव सहित विभिन्न प्रजातियों से कोशिकाओं को अस्वीकार नहीं है। अपने छोटे आकार भी कोशिकाओं या आर्थोपेडिक अनुप्रयोगों में प्रयोगात्मक scaffolds के संस्करणों की बहुत छोटी संख्या के परीक्षण के सभी देता है। कई murine आर्थोपेडिक मॉडल हड्डी स्थिरता 17,18 के विभिन्न डिग्री बर्दाश्त कि सूचना दी गई है। उन systeendochondral चिकित्सा 19 सूचित किया गया है, हालांकि इस तरह के बाहरी fixators और ताला लगा प्लेटों के रूप में स्थिरता का बहुत ही उच्च स्तर, में परिणाम है कि एमएस मुख्य रूप से intramembranous हड्डी बन जाना द्वारा चंगा। इसके विपरीत, इस तरह के unfixed या आंशिक रूप से निश्चित दिमाग़ी पिन को रोजगार के रूप में उन कुछ सूक्ष्म और / या मैक्रो-गति, की अनुमति उन है कि आम तौर पर endochondral हड्डी बन जाना 20,21 की एक विशेषता के साथ चंगा। विलंबित संघ या लंबी हड्डी की गैर संघ दोष की वजह से आवश्यक स्थिरीकरण के अतिरिक्त स्तर तक चूहों में प्राप्त करने के लिए विशेष रूप से कठिन हैं। हालांकि, दृष्टिकोण के एक नंबर इंटरलॉकिंग नाखून के साथ मस्तिष्क का पिन, ताला लगा प्लेट्स और बाहरी fixators 22 सहित सूचित किया गया है। इन प्रणालियों को आम तौर पर अच्छी तरह से काम करते हैं, लेकिन उनकी जटिल डिजाइन वे स्थापित करने के लिए तकनीकी रूप से चुनौतीपूर्ण हो सकता दी। उदाहरण के लिए, गार्सिया एट अल। 23 चूहों में उपयोग के लिए एक सुंदर इंटरलॉकिंग पिन प्रणाली तैयार है, लेकिन प्रक्रिया दो अलग-अलग स्थल पर चीरों शामिलs और फीमर की व्यापक संशोधन पिन समायोजित करने के लिए। इन प्रक्रियाओं के एक विदारक माइक्रोस्कोप के तहत प्रदर्शन किया गया।
इस के साथ साथ, हम एक 3 मिमी हड्डी घाटे का समापन रोकने के लिए और भी दोष के मूल किनारों को चित्रित करने के लिए डिजाइन एक केंद्रीय कॉलर के साथ एक सरल और्विक दिमाग़ी पिन का वर्णन है। पिन हड्डी खुद के लिए तय नहीं किया गया है, जबकि पर्याप्त हस्तक्षेप में दिमाग़ी गुहा परिणामों की पिन व्यास और Reaming की सटीक नौकरशाही का आकार घटाने मरोड़ गति (चित्रा 1) को कम से कम करने के लिए। जन्मजात उम्र, लिंग और तनाव-मिलान चूहों का चयन सावधानी के साथ, परिणाम आसानी से radiologically मूल्यांकन किया जा सकता है, जो एक बेहद प्रतिलिपि प्रस्तुत करने योग्य hypertrophic गैर uniondefect 22 है। इसके अलावा ब्याज के क्षेत्रों reproducibly डी नोवो हड्डी गठन और histomorphological मापदंडों की माप के लिए सूक्ष्म गणना टोमोग्राफी (μCT) के बाद से परिभाषित किया जा सकता है। पिन आसानी से उपलब्ध उपकरणों का उपयोग हमारी प्रयोगशाला में prototyped थे।
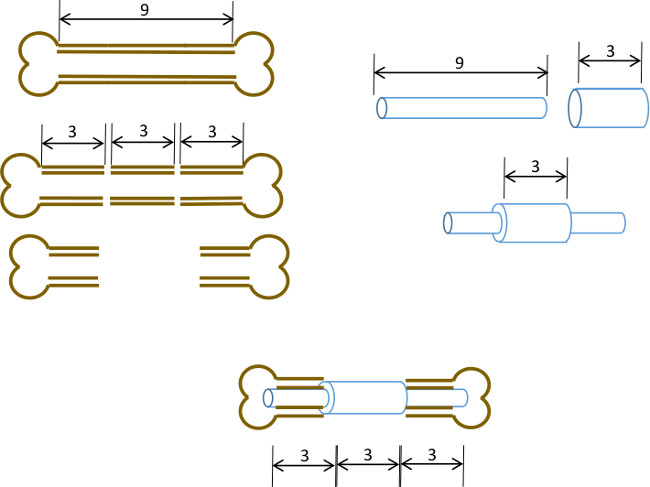
चित्रा 1: प्रायोगिक सिद्धांत कमानी दोष मॉडल के ढांचे के सारांश।। एक 9-10 मिमी murine फीमर के मध्य 3 मिमी खंड (बाएं) शल्य चिकित्सा excised है। एक 3 मिमी लंबा, 19 गेज शल्य स्टील ट्यूब सटीक केंद्र (दाएं) में लंबे समय से एक 9 एमएम, 22 ग्राम स्टेनलेस स्टील ट्यूब पर पारित किया है और चिपकने के साथ तय हो गई है। परिणामी पिन हड्डी के 3 मिमी खंड की जगह 19 जी कॉलर (नीचे, केंद्र) के साथ फीमर के शेष प्रॉक्सिमल और बाहर भाग के दिमाग़ी नहरों में लगाया जाता है।
