The characterization of the nine individuals studied, including their age, weight, height, and BMI, are shown in Table 1.
According to the cellular yield initially presented, the cell volume inoculated in culture was calculated to be as close as possible to the capacity of the 75 cm2 culture flask. The sample volume seeded in each case is described in Table 2. Then, according to the initial cellular yield, a variable volume of cells for each sample was determined: 1 mL for samples with higher cellular yield, 1.1 mL for samples with intermediate cellular yield, and 2 mL for samples with lower cellular yield so as to perform more similar cell seeding between cases. When the culture reached about 80%-90% confluence (Figure 2A) (about 7.5 ± 4.5 days), trypsinization of adherent cells was carried out (Table 2 and Figure 2B).
The cellular yield before passage 1 broadly varied even when the same confluence before trypsinization was observed (Table 2). This can be explained by the fact that cells may have grown in layers. Different parameters from the patients' ADSC were also assessed at different periods, as demonstrated in Table 2.
Some samples (Case 1, Case 2, Case 7) could not be evaluated regarding the percentage of confirmed ADSC and the estimated number of ADSC in culture due to bacteria contamination and lack of available cells to perform cryopreserved SVF immunophenotyping. According to the Spearman's Rho Calculator33, no statistical differences were found between SVF cellular yield and days to P1 (r = 0.37816, p = 0.31561), between SVF cellular yield before and after going to P1 (r = -0.33333, p = 0.38071), and between days to P1 and cellular yield before going to P1 (r = -0.53783, p = 0.13529). Furthermore, no significant differences were observed when correlating the SVF cellular yield with the average percentage of confirmed ADSC (r = -0.02857, p = 0.95716) and between the average percentage of confirmed ADSC and the cellular yield before going to P1 (r = 0.42857, p = 0.3965). Also, the correlation between BMI and SVF cellular yield could not be considered statistically significant (r = -0.46667, p = 0.20539). Table 3 shows flow cytometric data performed on SVF cells cryopreserved. The initial SVF cells contained a subset of positive cells for hematopoietic markers (CD45, CD11b, CD19, HLA-DR)34. From the initial SVF cell population, a particular subgroup expressed CD11b34 and CD1934 stromal cell-associated markers. The levels of CD7334, CD9034, and CD10534 were intermediate between these values. The initial SVF contained a subpopulation of cells positive for stem cell-associated markers (Figure 3). A mean of 79% of SVFs expressed the HSC-associated marker CD3434.
In total, 21 min were necessary for the three washes, 30 min for collagenase digestion, 10 min for centrifugation, and 5 min for cell counting and plating.
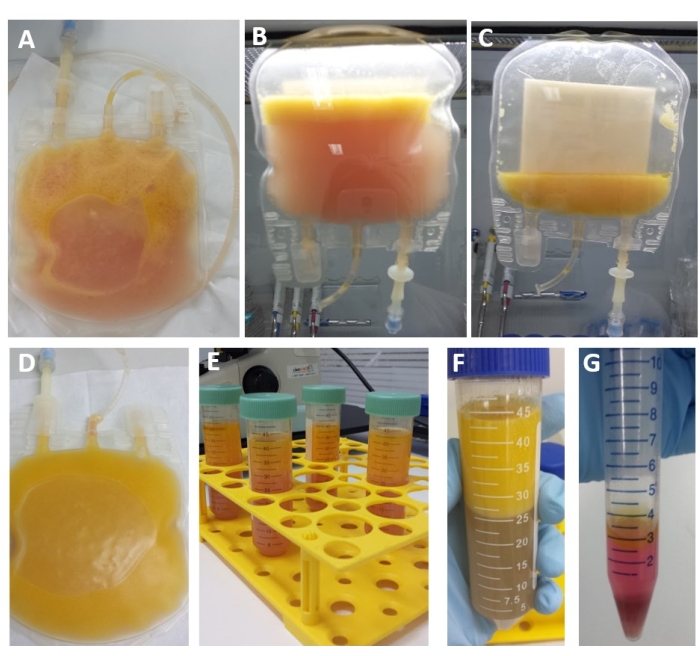
Figure 1: Steps from the protocol adipose-derived stem cells isolation. (A) Bag for lipoaspirate transport in a closed system. (B) The step of resting bag repeated three times, after washing. (C) Lipoaspirate after three washes with DPBS. (D) Lipoaspirate after collagenase digestion. (E) Lipoaspirate after digestion is distributed in a 50 mL tube. (F) Digested lipoaspirate after centrifugation. (G) Final process isolation with the pellet with the stromal vascular fraction (SVF). Please click here to view a larger version of this figure.
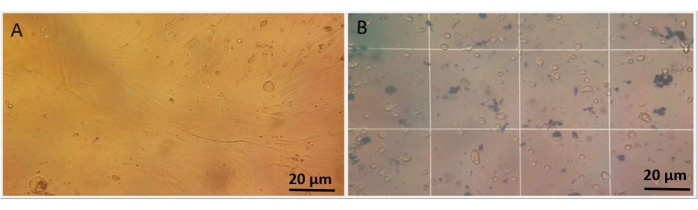
Figure 2: Morphology and viability of ADSCs. (A) Plastic adherent mesenchymal adipose-derived stem cells at the first passage after isolation at light microscopy. The cells show adhesion to the plastic and fibroblast-like morphology. (B) Trypan blue assay showing viable cells counted in Neubauer chamber using a light microscope. Please click here to view a larger version of this figure.
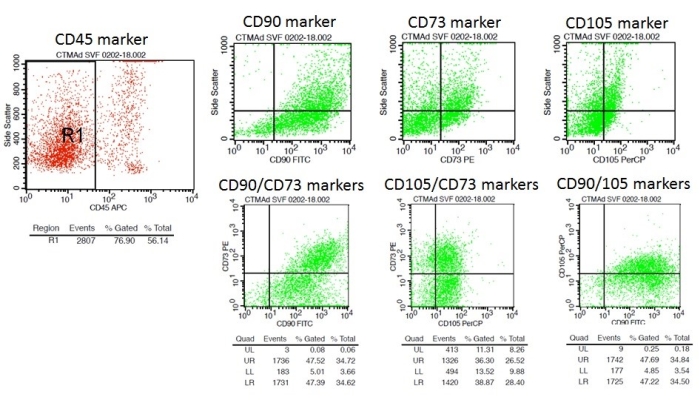
Figure 3: Subpopulation of cells positive for stem cell-associated markers in SVF of Case 9 after 8 months of cryopreservation. R1: Total cellular region analyzed in FSC (Forward Scatter) x SSC (Side Scatter) (Size x Complexity); R2: CD45 negative region, whose populations CD73, CD90, and CD105 are positive in this region. Please click here to view a larger version of this figure.
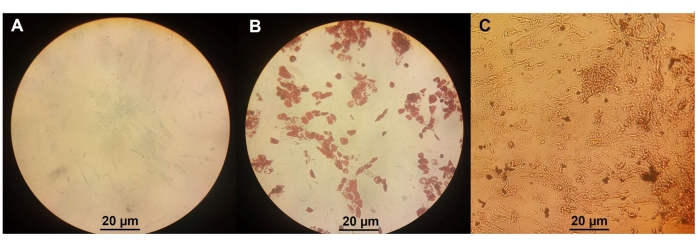
Figure 4: Differentiation assay. (A) ADSC differentiation in chondrocytes. (B) ADSC differentiation in osteocytes. (C) ADSC differentiation in adipocytes. Please click here to view a larger version of this figure.
| Patient | Age at collection (years) | Weight (kg) | Height (meter) | BMI* |
| Case 1 | 35 | 68 | 1.64 | 25.28 |
| Case 2 | 33 | 65 | 1.65 | 23.88 |
| Case 3 | 35 | 70 | 1.68 | 24.8 |
| Case 4 | 34 | 72 | 1.64 | 26.77 |
| Case 5 | 36 | 72 | 1.69 | 25.21 |
| Case 6 | 36 | 67 | 1.64 | 24.91 |
| Case 7 | 38 | 62 | 1.53 | 26.49 |
| Case 8 | 50 | 63 | 1.68 | 22.32 |
| Case 9 | 37 | 65 | 1.58 | 26.04 |
Table 1: Data from the samples of the individuals studied. *BMI: body mass index.
| Patient | Volume collected (mL) | SVF Cellular yield (cell/mL) (x 105) | Volume in culture (mL) | Average percentage of confirmed ADSC (%) | Number of cells in initial culture (x 105) | Estimated number of ADSC in culture (x 105) | Days to P1 | Cellular yield before going to P1 (x 105) |
| Case 1 | 96 | 9.2 | 2 | na | 18.4 | na | 10 | 18 |
| Case 2 | 100 | 25.2 | 1 | 38 | 25.2 | 9.6 | 12 | 10.8 |
| Case 3 | 100 | 26.2 | 1 | na | 26.2 | na | 12 | 6.6 |
| Case 4 | 105 | 21.1 | 1 | 55.9 | 21.1 | 11.8 | 3 | 13.1 |
| Case 5 | 110 | 23.7 | 1 | 61.4 | 23.7 | 14.5 | 4 | 16.1 |
| Case 6 | 100 | 13.3 | 1.1 | 78.9 | 14.6 | 11.5 | 10 | 13.5 |
| Case 7 | 98 | 6.8 | 2 | na | 13.6 | na | 8 | 10.5 |
| Case 8 | 100 | 9.7 | 1.1 | 44.2 | 10.7 | 4.7 | 11 | 6.9 |
| Case 9 | 100 | 6.1 | 2 | 43.8 | 12.2 | 5.3 | 6 | 15.9 |
| SD | 3.89 | 7.81 | 0.46 | 13.75 | 5.55 | 3.53 | 3.2 | 3.79 |
Table 2: Data from different steps of the procedure from the nine patients analyzed. SVF: stromal vascular fraction; ADSC: adipose-derived stem cell; P1: passage 1; na: data not available.
| SAMPLE | % Of ADSC DETERMINED BY MONOCLONAL ANTIBODIES | % OF HEMATOPOIETIC CELLS DETERMINED BY MONOCLONAL ANTIBODIES | CELL VIABILITY ASSAY AND TIME OF SVF CRYOPRESERVATION | |||||||||
| CD45-(*) | CD73+/CD90+ | CD73+/CD105+ | CD105+/CD90+ | Mean | CD34+ | HLA-DR+ | CD11b+ | CD19+ | LIVE/DEAD + | |||
| Case 2 | 52.34% | 31.97% | 25.36% | 56.52% | 37.95% | 63.16% | 12.87% | 2.41% | 0.21% | 39.54% (2 years) | ||
| Case 4 | 48.02% | 61.62% | 40.93% | 65.25% | 55.93% | 82.94% | 26.62% | 0.00% | 0.16% | 38.30% (2 years) | ||
| Case 5 | 27.74% | 54.02% | 49.72% | 80.42% | 61.38% | 73.33% | 51.31% | 0.05% | 0.00% | 23.06% (2 years) | ||
| Case 6 | 55.52% | 79.52% | 67.70% | 89.52% | 78.91% | 86.86% | 8.83% | 0.18% | 1.06% | 56.76% (2 years) | ||
| Case 8 | 57.28% | 46.84% | 30.88% | 57.65% | 45.12% | 78.47% | 26.97% | 0.03% | 0.00% | 55.56% (1 year) | ||
| Case 9 | 56.14% | 47.52% | 36.30% | 47.69% | 43.83% | 88.10% | 26.94% | 0.05% | 0.24% | 72.34% (8 months) | ||
Table 3: Flow cytometry data from six of the patients. (*) From these CD45- cells, % of ADSC with different combinations of stem cell markers was determined. ADSC: adipose-derived stem cell; SVF: stromal vascular fraction; (*) From these CD45- cells, % of ADSC with different combinations of stem cell markers was determined.
