From 2020 to 2022, six patients with HCC underwent fluorescent laparoscopic central hepatectomy. Among these, four patients underwent resection of segments 4, 5, and 8, and two patients underwent resection only of segments 5 and 8 (Table 1). None of the patients were converted to open surgery. Their ages ranged from 46 to 74 years. The tumor sizes ranged from 5 to 9 cm. The median operative time was 240 min, and the median intraoperative blood loss was 450 mL. The median postoperative hospital stay was 7 days. All patients are still under follow-up.
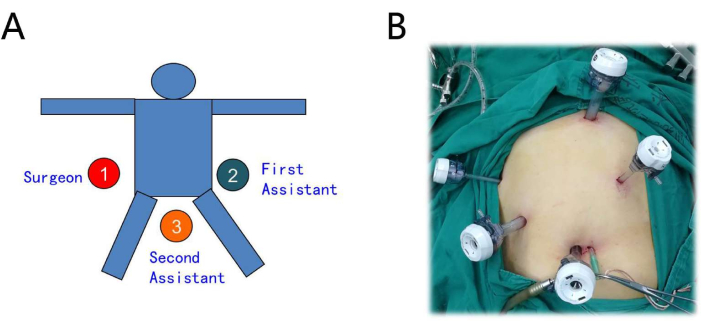
Figure 1: Setting of the patient and trocar layout. (A) The operator is on the right, the first assistant on the left, and the second assistant between the legs. (B) The procedure is performed using a five-port technique. Please click here to view a larger version of this figure.
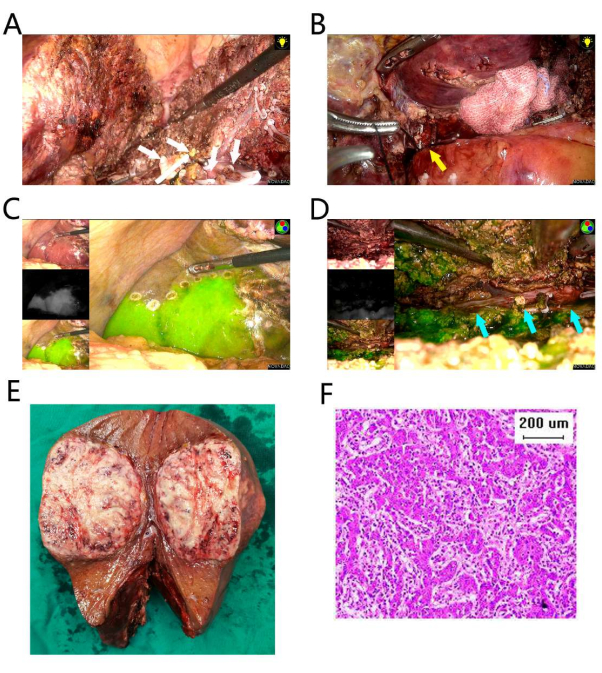
Figure 2: Resection of segments 4, 5, and 8. (A) The liver resection of the left plane was processed first. Several branches of the segment 4 Glisson pedicle were ligated and transected (white arrows). (B) The right anterior hepatic pedicle was separated and ligated (yellow arrow). (C) The fluorescent border is on the right side. (D) The liver parenchyma was dissected along the right fluorescent border, and the RHV was exposed (blue arrows). (E) The resection specimen. (F) Pathology of hematoxylin and eosin (HE) staining suggests poorly differentiated HCC. The scale bar is 200 µm. Please click here to view a larger version of this figure.
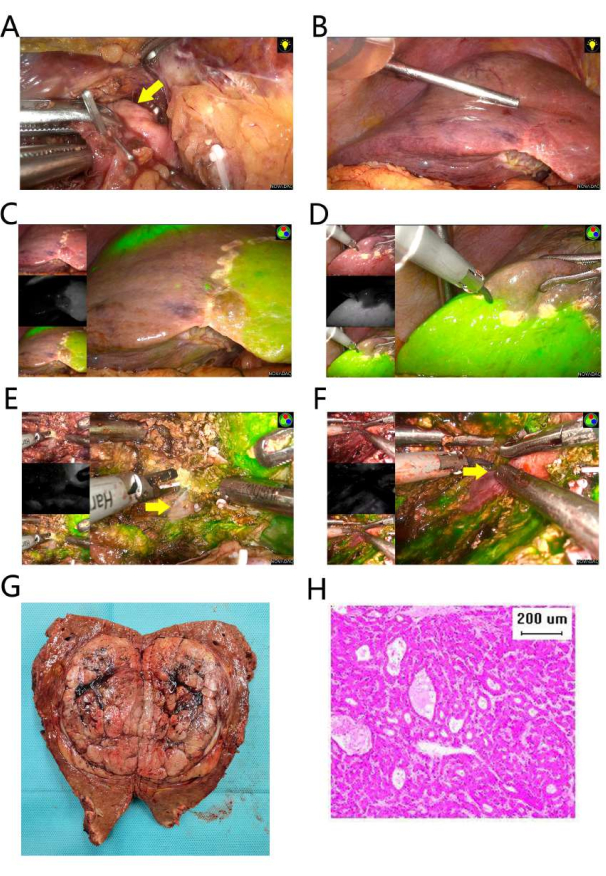
Figure 3: Resection of segments 5 and 8. (A) The right anterior hepatic pedicle was separated and ligated (yellow arrow). (B) Ischemia of right anterior section. (C) The fluorescent border is on the left side. (D) The fluorescent border is on the right side. (E) The liver parenchyma was dissected along the left fluorescent border, and the MHV was exposed (yellow arrow). (F) The liver parenchyma was dissected along the right fluorescent border, and the RHV was exposed (yellow arrow). (G) The resection specimen. (H) Pathology of HE staining suggests moderately differentiated hepatocellular carcinoma. The scale bar is 200 µm. Please click here to view a larger version of this figure.
| Case | Type of operation | Gender | Age (years) | Tumor Size (cm) | Operation Duration (min) | Blood Loss (mL) | Post- operative biliary fistula |
Liver dysfunction | Post- operative Hospital Stay (day) |
| 1 | S4,5,8 | M | 74 | 9 | 420 | 800 | No | No | 7 |
| 2 | S4,5,8 | M | 46 | 6 | 240 | 800 | No | No | 7 |
| 3 | S4,5,8 | M | 62 | 5 | 180 | 50 | No | No | 6 |
| 4 | S4,5,8 | M | 74 | 7 | 240 | 50 | No | No | 7 |
| 5 | S5,8 | M | 73 | 8 | 180 | 100 | No | No | 7 |
| 6 | S5,8 | M | 61 | 6 | 540 | 800 | No | No | 7 |
Table 1: Clinical parameters of the six patients.
